
A late-night search for best outpatient rehab near me usually starts the same way. A spouse is awake long after everyone else is asleep. A parent has too many tabs open. The person who needs help may be saying they cannot disappear for a month, cannot leave work, or cannot step away from children and daily responsibilities.
That is why outpatient treatment matters. It gives people a real way to get help while staying connected to ordinary life.
The search still feels confusing. Many websites say the same things, few explain the trade-offs clearly, and almost none tell families how to judge whether a program is equipped to treat both addiction and mental health together. Clear answers matter because treatment demand has been rising for years. In Miami-Dade County, admissions for drug addiction treatment rose from 9,877 in 2012 to 26,713 in 2016, a sharp increase that highlights the need for accessible outpatient care in large metro areas (Miami-Dade addiction treatment data).
Finding Hope in Orange County When You Feel Lost
Orange County families often reach this point after weeks or months of trying to manage things on their own. Someone promises to cut back. A rough weekend passes. Work performance slips. Anxiety gets worse. Alcohol, pills, or other substances stop looking like the main problem and start looking tied to depression, trauma, panic, or burnout.
That is where many online searches go wrong. Families look for the “best” program, but what they really need is the right level of structure and the right clinical fit.
Why the search feels so hard
Most treatment websites focus on comfort, location, or broad promises. Those details matter, but they do not answer the hard questions:
- Can this program treat mental health and substance use together
- Will the schedule fit around work, parenting, or school
- Is medication support available when it is clinically appropriate
- Will the person have support after the most intensive phase ends
A good admissions conversation should clear this up quickly. It should ask about substance use, mental health symptoms, safety concerns, prior treatment, home support, and whether the person can stay stable outside a residential setting.
A useful rule for families is simple. If a program cannot explain who belongs in each outpatient level of care, that program is not making the process easier.
What families need
Families do not need another generic list. They need a way to sort through choices with confidence.
In Orange County, that means looking for a program that offers more than a weekly therapy appointment. It means finding a structured path, starting with the right intensity, then stepping down carefully as stability improves. It also means choosing a team that can address the practical realities of life in recovery, including transportation, scheduling, family involvement, and the emotional crash that often comes after detox or inpatient discharge.
When the search is framed that way, the next step becomes much clearer.
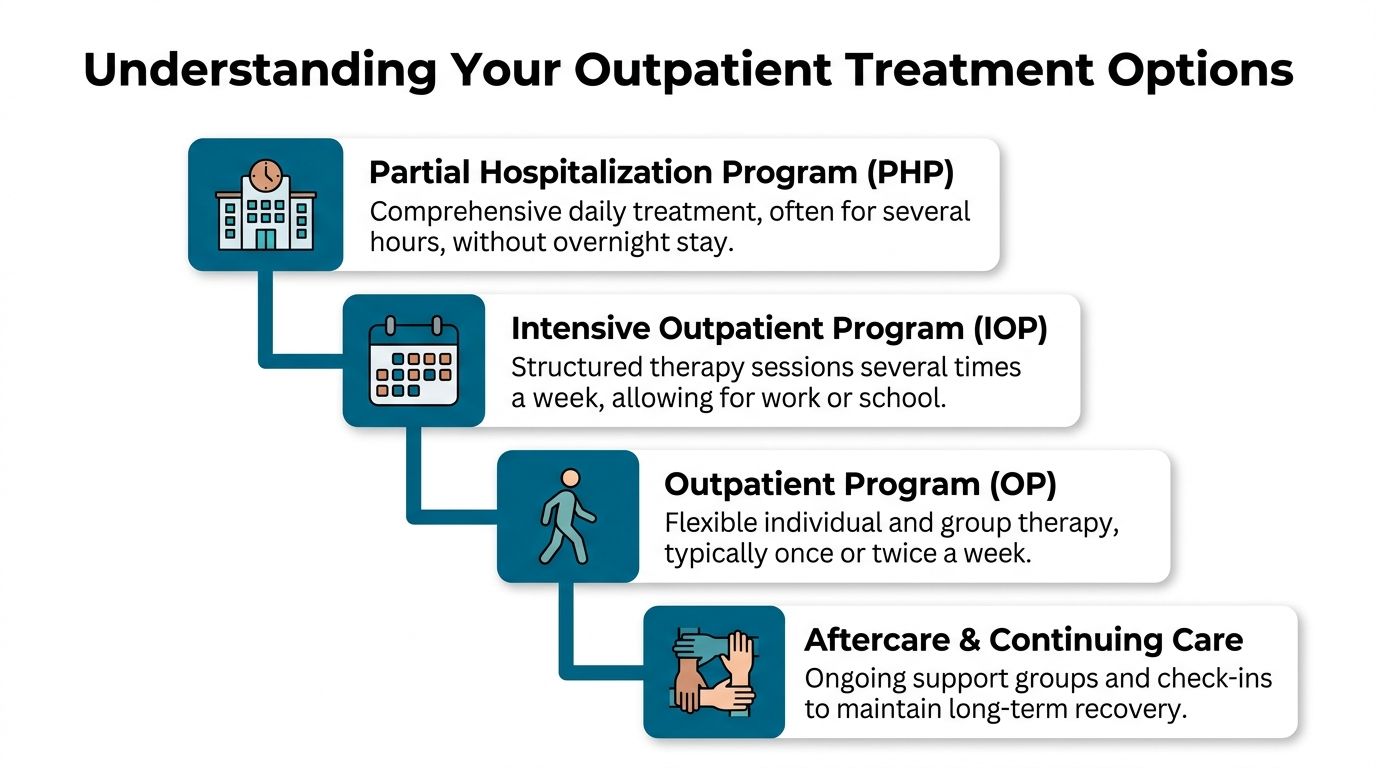
Understanding Your Outpatient Treatment Options
Outpatient care works best when families understand that it is not one single service. It is a continuum. The easiest way to think about it is like physical rehabilitation after an injury. Some people need daily support at first. Others can start with a few structured sessions each week. As strength returns, the treatment schedule gets lighter, but support does not disappear.
Outpatient treatment is also much more accessible for many households. Standard outpatient programs average $8,295, compared with nearly $50,000 for long-term inpatient care, and 60% of patients transitioning from detox prefer outpatient options that let them maintain work and family life (outpatient rehab cost and transition preferences).
The main levels of care
Partial Hospitalization Program or PHP
PHP is the highest outpatient level. It usually involves treatment for several hours a day on multiple days each week, without an overnight stay. This level often fits people leaving detox or residential care, or people who need intensive daily structure but are safe sleeping at home or in supportive housing.
Intensive Outpatient Program or IOP
IOP is a step down from PHP, but it is still structured and serious. It commonly includes several therapy sessions each week and gives people room to keep working, attend school, or meet family responsibilities. For many adults searching best outpatient rehab near me, IOP is the level that balances accountability with day-to-day life. A practical example of this model appears in this overview of an intensive outpatient program IOP rehab.
Outpatient Program or OP
OP is less intensive. It usually includes individual therapy, group therapy, or both, on a flexible schedule. This level often works as a maintenance phase after PHP or IOP, or for people whose needs do not require a heavier structure.
Aftercare and continuing care
Recovery does not end when the formal program hours decrease. Continuing care can include alumni check-ins, relapse prevention planning, family support, and regular clinical follow-up.
A quick comparison
| Program Level | Time Commitment | Best For |
|---|---|---|
| PHP | Several hours a day, multiple days a week | People needing strong daily structure without overnight stay |
| IOP | Several sessions a week | People balancing treatment with work, school, or family responsibilities |
| OP | Flexible weekly sessions | People stepping down from higher care or needing lighter ongoing support |
How to tell where someone belongs
Placement should never be based on convenience alone.
A strong clinical assessment looks at:
- Current stability: Whether cravings, withdrawal risk, or recent use require more structure.
- Mental health needs: Whether depression, trauma, anxiety, or mood swings are affecting safety and recovery.
- Home environment: Whether the person has support, accountability, and a reasonably stable place to live.
- Treatment history: Whether past attempts failed because support was too light.
When the level of care matches the person, outpatient treatment becomes much more than a compromise. It becomes a practical, sustainable way to build recovery.
The Undeniable Hallmarks of a Top-Tier Rehab Program

Not every outpatient program is built the same way. Some offer a thin schedule, generic groups, and little follow-through. Others are organized around what helps people stay engaged long enough to stabilize, address underlying issues, and build a recovery routine that can survive real life.
Three markers separate strong programs from weak ones.
Dual-diagnosis care is not optional
A person may start treatment because of alcohol, opioids, stimulants, or prescription medication misuse. Once treatment begins, another layer often becomes impossible to ignore. Panic symptoms. Trauma reactions. Depressive crashes. Obsessive thinking. Sleep disruption. Emotional volatility.
If a program treats substance use while ignoring mental health, families usually see the same cycle repeat. The person may stop using for a short period, but the untreated distress remains. Sooner or later, the old coping pattern returns.
Dual-diagnosis care means the treatment plan addresses both sides at the same time. That should include psychiatric evaluation when appropriate, individual therapy, group work, and practical skill-building that helps the client manage triggers, relationships, and emotional regulation.
A useful question for any admissions team is straightforward. Ask how the program adjusts treatment when the person has both addiction and a mental health condition. A vague answer is a warning sign.
MAT should be available when clinically appropriate
Medication-Assisted Treatment (often called MAT) matters most when a person is dealing with opioid or alcohol dependence and needs more than counseling alone. In Southern California, 65% of accredited facilities now incorporate MAT, and those programs show 55% to 70% retention rates at 6 months, while also outperforming non-MAT programs by 40% in reducing relapse for opioid and alcohol dependencies (Southern California MAT and retention data).
Those numbers matter because retention matters. A program cannot help a person who drops out after the first few difficult weeks.
Families should not ask whether medication is good or bad in the abstract. They should ask whether the clinical team knows when medication belongs in the plan, how progress is monitored, and how therapy and medication work together.
MAT is not a shortcut. It is one evidence-based option within a larger treatment strategy. The strongest outpatient programs explain this clearly and without stigma.
Whole-person care should support treatment, not replace it
Many families hear terms related to overall well-being and become skeptical, often for good reason. In weaker settings, approaches focused on overall well-being are used as a substitute for solid clinical work. It becomes branding instead of treatment.
In a strong program, extensive well-being support plays a different role. It helps people relearn regulation, routine, and body awareness. That can include yoga, nutrition guidance, experiential activities, movement, and outdoor work that supports emotional steadiness. Some people also benefit from structured movement practices that improve posture, breath control, and physical self-awareness. This overview of Pilates for rehabilitation gives a useful example of how movement can be part of recovery support when used thoughtfully.
Elements supporting overall well-being work best when they are tied to a clear clinical purpose. A person with anxiety may need grounding skills. A person with depression may need gradual activation and structure. A person recovering from prolonged substance use may need help reconnecting with physical health in a manageable way.
Small groups and individualized planning matter
Families often assume more hours automatically mean better treatment. That is not always true.
A better question is whether the client is known by the team. In strong outpatient care, groups do not feel anonymous, case management follows through, and individual sessions connect to the specific problems the client is facing outside the building. That includes work pressure, family conflict, court issues, unstable housing, or the difficult social shift that comes with early sobriety.
This is also where evidence-based treatment needs to be more than a buzzword. Families who want a grounded overview of what that term should mean can review this resource on evidence-based treatment approaches.
What quality looks like in practice
A high-quality outpatient program should be able to answer these questions clearly:
- Assessment: How does the team decide between PHP, IOP, and standard outpatient?
- Mental health integration: What happens if depression, trauma, or anxiety is driving substance use?
- Medication access: Is MAT available when it fits the diagnosis and recovery plan?
- Family support: How are loved ones included without turning treatment into constant crisis management?
- Step-down planning: What support exists when the person finishes the most intensive phase?
One Orange County option that fits this framework is Zoe Behavioral Health, an outpatient program in Lake Forest that offers PHP, IOP, outpatient counseling, dual-diagnosis care, broad well-being support, and alumni engagement.
The right program should not just offer services on a menu. It should show how those services fit together around the person.
What to Expect A Day in Outpatient Treatment

One reason people hesitate to enter outpatient rehab is that they cannot picture what the day will feel like. They imagine something cold, rigid, or overwhelming. In a well-run program, the day is structured, but it is not chaotic or punishing.
The rhythm of the day
A typical outpatient day often begins with check-in. The client arrives, settles in, and reconnects with the treatment environment. That opening matters. It helps the clinical team notice changes in mood, stress level, cravings, or engagement before the rest of the day unfolds.
From there, the schedule usually blends several elements:
- Group therapy: Clients work through triggers, coping patterns, communication issues, relapse prevention, and emotional regulation.
- Individual sessions: A therapist focuses on the client’s personal history, goals, setbacks, and mental health concerns.
- Skills-based work: Clients practice routines they can use at home, not just ideas they discuss in session.
- Case management or family coordination: Staff help with practical barriers that can derail recovery.
The strongest programs keep the day active enough to create momentum, while still leaving room for reflection and personal accountability.
What group therapy feels like
Many people fear group therapy before they attend it. They expect pressure, judgment, or forced disclosure. Well-facilitated groups feel different.
Clients hear from others facing similar patterns, which often lowers shame quickly. They also begin to notice the stories they tell themselves. Excuses become easier to spot. So do strengths.
A good group does not push people to perform recovery. It teaches them how to practice honesty, boundaries, and accountability in real time.
Why continuing support matters
The most important outpatient question is not whether someone can attend for a few weeks. It is whether support continues long enough to help recovery hold after the initial push of treatment fades.
That is why alumni and continuing care matter. Outpatient completion rates average 40% to 60%, but programs with strong alumni engagement can achieve 25% higher 6-month sobriety rates, a benefit many families never see explained clearly when comparing programs (outpatient completion and alumni outcome data).
A typical week in treatment should not feel like isolated appointments. It should feel like a connected process, with each session building on the last and preparing the client for the hours when treatment is over and ordinary life resumes.
The practical side families often overlook
A day in outpatient care still leaves room for real life. Clients may return home, go to work, attend family obligations, or rebuild routines around sleep, meals, exercise, and sober support. That is part of the value.
The person is not practicing recovery in a bubble. The person is practicing it where life happens.
Navigating Admissions and Insurance Without the Headache
For many families, admissions is the most stressful part of the process. They are ready to act, but then they hit the usual obstacles. Insurance confusion. Questions about prior authorization. Fear of hidden costs. Uncertainty about what records are needed. Delays while everyone waits for someone else to call back.
That stress is not minor. In California, 40% of outpatient claims can be denied for “medical necessity,” and centers that provide 24/7 insurance verification can cut admission delays by 70% (California outpatient insurance denial and verification data).
What the admissions process should look like
A clean admissions process usually follows a simple sequence.
Initial call
The team gathers a brief history of substance use, mental health symptoms, recent treatment, and current safety concerns.Clinical screening
Staff determine whether outpatient care fits, or whether detox, residential support, or a higher level of care is needed first.Insurance verification
Benefits are checked before admission so families understand coverage, likely responsibilities, and any authorization needs.Scheduling
The program coordinates the intake and start date as quickly as possible.
A family dealing with this process for the first time can benefit from a practical admissions overview such as this guide on how to find help for substance abuse admissions.
Questions to ask before saying yes
Not every admissions call is equally helpful. Families should ask direct questions.
- Coverage clarity: What is known about insurance benefits today, and what still needs verification?
- Level of care: Why is this person being recommended for PHP, IOP, or outpatient?
- Documentation: Will the program help gather what is needed for medical necessity review?
- Start timeline: How fast can the intake happen if the person is ready now?
If an admissions team avoids specifics about insurance or cannot explain why a certain level of care was recommended, families should slow down and ask more questions.
The right admissions process lowers confusion. It does not add to it.
Frequently Asked Questions About Outpatient Rehab
Can someone keep working while in treatment
Often, yes. That is one of the main reasons outpatient care works for so many adults. The schedule depends on the recommended level of care. A higher level like PHP requires more daytime availability. IOP and standard outpatient usually offer more room to keep up with employment, school, or family responsibilities.
The key issue is not just time. It is whether the current work environment supports recovery or keeps triggering the same behavior.
Is outpatient rehab enough for serious addiction
Sometimes it is. Sometimes it is not.
Outpatient works well when the person is medically stable, can remain safe outside a residential setting, and has enough support and accountability to follow through. If someone is in active withdrawal, has repeated immediate relapse after short periods of abstinence, or cannot stay safe at home, a higher level of care may need to come first.
What role should family play
Family involvement helps when it is structured. Loved ones can support treatment by learning about boundaries, communication, enabling patterns, and realistic expectations. They should not be turned into full-time monitors.
Good outpatient care gives families a place to participate constructively without making them responsible for the outcome.
Is sober living required
No. It depends on the person’s environment.
Some people do well sleeping at home and attending treatment during the day. Others need a more recovery-focused living setting because home is unstable, isolating, or full of triggers. Sober living can be helpful when it adds accountability and routine, but it should fit the clinical picture, not be treated as automatic.
How does someone know a program is the right fit
The answer should come from the assessment, not from marketing language.
A strong fit usually means the program can explain the recommended level of care, address both addiction and mental health, involve family appropriately, help with insurance, and provide a path for continuing support after the initial phase of treatment.
When families search best outpatient rehab near me, the best next move is often a direct conversation with an admissions team that can evaluate the situation clearly and respond quickly. Delay tends to make the situation harder, not easier.
For anyone in Orange County who is weighing options and needs a clear clinical path, Zoe Behavioral Health offers admissions guidance, insurance verification, and outpatient treatment planning for substance use and co-occurring mental health needs. A single phone call can clarify level of care, timing, and next steps.