
A common California recovery story often starts. A person feels anxious, low, overwhelmed, or unable to sleep. Alcohol, pills, or another substance seems to take the edge off for a few hours. Then the rebound arrives. Anxiety gets louder, mood drops further, relationships strain, and the substance starts looking less like relief and more like survival.
Families often misread this cycle. They may see only the drinking, only the panic, or only the depression. In many cases, both conditions are feeding each other at the same time. That is why the search for dual diagnosis treatment centers california matters so much. The goal is not just to stop substance use for a few days. The goal is to build a treatment plan that addresses the full picture and supports the return to ordinary life without losing ground.
The Dual Diagnosis Challenge in California
A person with dual diagnosis lives with both a substance use disorder and a mental health condition at the same time. One problem can intensify the other.
An adult may drink to quiet social anxiety. Another may misuse opioids while struggling with trauma symptoms. Someone else may use stimulants to push through depression and then crash harder afterward. This is not a character issue. It is a clinical pattern that requires integrated care.
What dual diagnosis looks like in real life
The confusion usually comes from timing.
Sometimes the mental health symptoms came first, and substance use became a form of self-medication. Sometimes substance use escalated first and then triggered intense anxiety, depression, paranoia, or emotional instability. Sometimes nobody can tell which began first because both are now tightly woven together.
That is why separate, disconnected treatment often falls short. If one provider treats only the addiction while another treats only the mood symptoms, the patient can end up carrying the burden of coordination during the most vulnerable period of recovery.
For many families, the first moment of clarity comes when they learn how common co-occurring disorders are. In California, 34.4% of county mental health service clients in 2015 had co-occurring mental health and substance use disorders, and 8.5% of all Californians were estimated to experience these disorders, according to California dual diagnosis treatment data.
Why so many people feel stuck
Dual diagnosis can feel like trying to put out a fire while someone keeps adding fuel from another room.
A person may attend therapy but keep drinking every night to sleep. Another may stop using for a short stretch but feel such severe anxiety or hopelessness that relapse starts to feel inevitable. This overlap is why many people say they have “tried treatment before” and still do not feel understood.
The relationship between mental health and substance use is not abstract. It shows up in missed work, isolation, family conflict, medication confusion, and repeated crises. A plain-language overview of the connection between mental health and addiction can help families understand why the cycle keeps repeating.
Key takeaway: When substance use and mental health symptoms rise and fall together, the treatment plan has to address both at the same time.
Why Integrated Treatment is the Only Path Forward
Treating co-occurring disorders separately is like repairing two locked gears in a machine while pretending they do not touch. One gear turns the other. If only one gets repaired, the system still grinds, slips, and breaks down under pressure.
That is the practical reason integrated treatment matters. It does not split a person into “the addiction problem” and “the mental health problem.” It treats the person as one whole clinical picture.
Why separate treatment creates setbacks
Consider a patient with panic symptoms and heavy alcohol use.
If treatment focuses only on stopping alcohol, the panic may surge once alcohol is removed. The patient may feel worse before new coping skills are in place. If treatment focuses only on anxiety but ignores active substance use, therapy can stall because the brain and body stay in a repeated cycle of intoxication, withdrawal, craving, and emotional instability. Consequently, many families get discouraged.
They assume treatment “did not work,” when in reality the treatment model was incomplete.
A landmark national study found that only 18% of addiction treatment programs were equipped for dual diagnosis capable services, meaning a patient has less than a 1-in-5 chance of finding a facility prepared for integrated care, according to the national study on dual diagnosis capability.
What integrated care means
Integrated treatment is not a buzzword. It usually includes one coordinated plan across several moving parts:
- Psychiatric care: Assessment of anxiety, depression, trauma-related symptoms, mood instability, or other mental health concerns.
- Addiction treatment: Therapy, relapse prevention work, substance use education, and accountability around recovery goals.
- Medication management: Review of current medications, side effects, misuse risk, and how medications fit the recovery plan.
- Behavioral therapies: Structured work on triggers, thought patterns, emotional regulation, and coping skills.
- Care coordination: Communication between clinicians so the patient is not repeating the same story to disconnected providers.
When these elements work together, treatment becomes more stable and more believable to the person receiving it. The patient no longer has to guess whether anxiety is causing relapse, whether relapse is worsening depression, or whether a medication change belongs to one provider or another.
The foundation for lasting progress
Integrated treatment creates the conditions for recovery by reducing chaos.
Instead of asking a struggling person to solve everything at once, it helps in sequence. First comes stabilization. Then the patient builds insight into patterns. Then therapy becomes more productive because the mind is less hijacked by craving, withdrawal, shame, or untreated psychiatric symptoms. Finally, the person practices recovery in everyday life with support still in place.
A strong dual diagnosis program tends to ask better questions than a standard program:
- What symptoms show up before substance use?
- What happens emotionally after use stops?
- Which triggers are psychiatric, which are environmental, and which are both?
- What level of structure does daily life require right now?
Those questions matter because dual diagnosis recovery is rarely about one dramatic breakthrough. It is usually about many well-coordinated decisions that help a person become safer, steadier, and more functional over time.
Clinical insight: Recovery becomes more durable when one team tracks the whole pattern instead of treating mental health and substance use as separate stories.
Navigating the Levels of Care from Detox to Daily Life
Few people need a vocabulary lesson when they are in crisis. They need a map.
Terms like detox, PHP, IOP, and outpatient can sound technical, but the basic idea is simple. Treatment usually works best when support matches the person’s current level of instability. As the person gains footing, care steps down gradually instead of disappearing all at once.
The treatment path in plain language
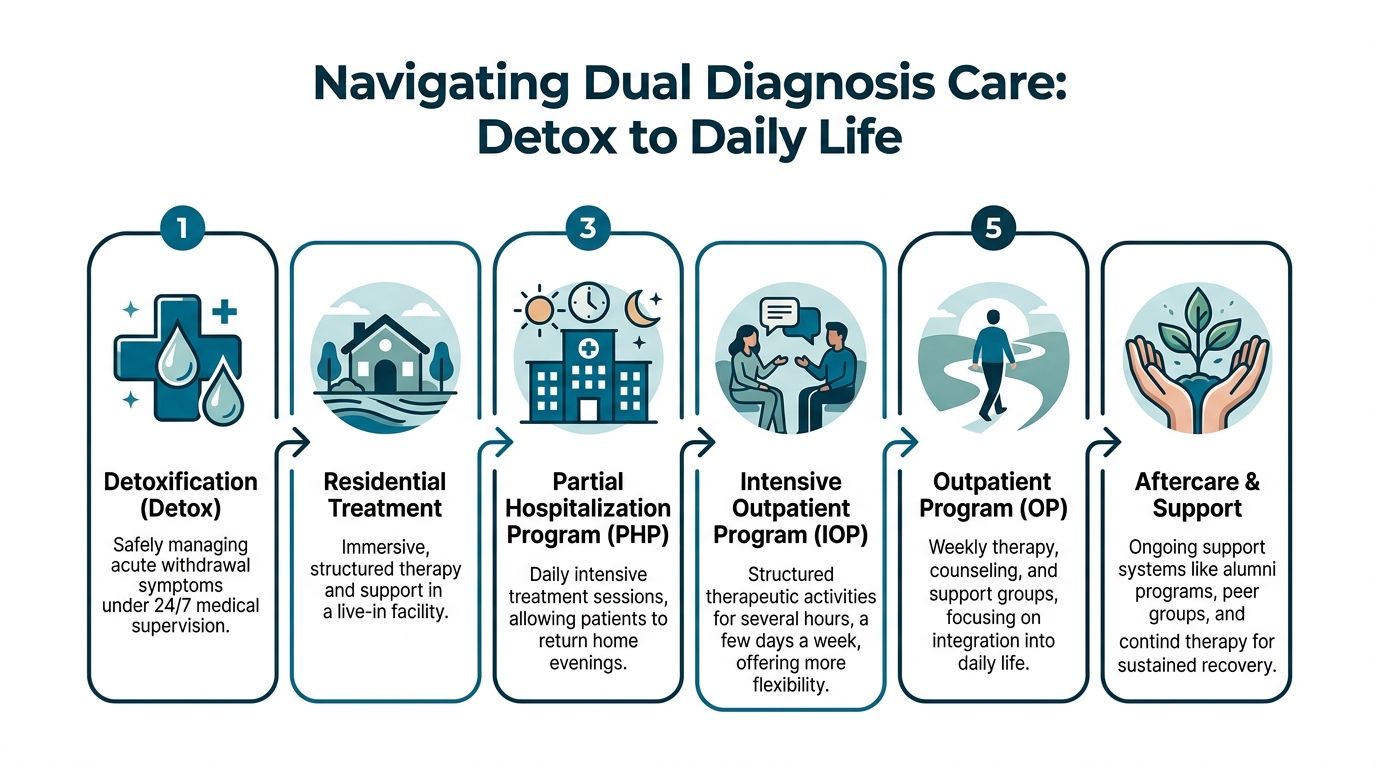
Detox is the first stop when withdrawal risk is significant. The job of detox is stabilization. It is not the same as full treatment. It helps the body clear substances safely and manages acute symptoms under medical supervision. For readers trying to understand what detox does and does not do, this overview on demystifying detox can clarify the process.
Residential treatment provides a live-in setting with high structure. This level can help when home life is unstable, relapse risk is high, or psychiatric symptoms need close monitoring within a contained environment.
PHP, or Partial Hospitalization Program, offers intensive treatment during the day while allowing the person to return home or to supportive housing in the evening. This level often fits people who need strong clinical structure but do not require inpatient living.
IOP, or Intensive Outpatient Program, is a step down from PHP. It provides meaningful therapeutic structure several days a week while allowing more room for work, school, family duties, and real-world practice.
Outpatient care is less intensive. It often includes individual therapy, group support, medication management, and ongoing relapse prevention while the person rebuilds routines.
Aftercare and support continue the process with alumni contact, peer support, therapy check-ins, and recovery planning. This phase matters because early recovery does not end when a formal program becomes less frequent.
Comparing outpatient levels of care
| Level of Care | Typical Weekly Hours | Primary Focus |
|---|---|---|
| PHP | Daily intensive schedule | Stabilization, symptom management, structure |
| IOP | Several hours on multiple days | Skill-building, relapse prevention, reintegration |
| Outpatient Program | Weekly or ongoing sessions | Maintenance, accountability, long-term recovery |
Where people often get lost
The biggest misunderstanding is this. People assume success depends on getting through detox or finishing a highly structured phase. In reality, many setbacks happen later, when the person returns to regular responsibilities while still feeling emotionally raw.
That step-down period can be difficult because daily life brings back the exact triggers treatment has identified: conflict at home, loneliness, commute stress, work pressure, sleep disruption, old social circles, and access to substances. Without support during that transition, motivation can collapse quickly.
Why step-down care matters so much
A good continuum of care works like training wheels that come off gradually.
PHP can hold someone steady while sleep, mood, cravings, and medication plans begin to stabilize. IOP can then help the same person test coping skills in ordinary life while still receiving substantial support. Standard outpatient care helps maintain momentum after the higher-risk phase has passed.
This is often the missing middle in recovery. The person is no longer in crisis, but also not fully secure. That middle period needs structure, observation, and flexibility.
A coordinated outpatient center can make that transition smoother by handling practical concerns such as:
- Medication follow-up: Psychiatric medications and recovery medications often need monitoring as routines change.
- Schedule planning: Work hours, childcare, transportation, and therapy attendance must fit real life.
- Relapse prevention: Triggers become clearer once the person returns to ordinary settings.
- Family communication: Loved ones may need coaching on boundaries, support, and warning signs.
- Sober living coordination: Some patients benefit from additional housing support while stepping down.
One outpatient model that addresses this gap is Zoe Behavioral Health in Lake Forest, which provides referrals to medical detox along with PHP, IOP, outpatient counseling, and sober living coordination from a single center. That kind of continuity can reduce the confusion that often appears when patients move between separate providers.
Practical point: The safest question is not “What program comes first?” It is “How will care continue when life starts demanding more from the patient again?”
Evidence-Based Therapies That Heal Mind and Body
People often hear that a center uses “evidence-based treatment” without being told what that means in daily practice. The term refers to therapies and medical approaches that clinicians use because they have a strong clinical foundation and a clear role in recovery.
For dual diagnosis treatment, those methods need to do two jobs at once. They must reduce substance use risk and help the person function better emotionally.
How therapy changes the pattern
Cognitive Behavioral Therapy (CBT) helps patients notice the link between thoughts, feelings, and actions.
A simple example helps. A patient thinks, “Nothing is getting better.” That thought triggers hopelessness. Hopelessness increases the urge to use. In CBT, the therapist does not offer empty reassurance. The therapist helps the patient test the thought, examine the evidence, and build a more useful response. That creates space for a different action.
A focused explanation of cognitive behavioral therapy for relapse prevention can help readers understand why this approach is so common in addiction and mental health care.
DBT, or Dialectical Behavior Therapy, often helps patients who struggle with intense emotions, impulsive behavior, or unstable relationships. It teaches concrete skills such as distress tolerance, emotional regulation, mindfulness, and interpersonal effectiveness.
These therapies are effective partly because they are practical. Patients do not just talk about life. They learn how to survive difficult moments without returning to old habits.
The role of medication in dual diagnosis treatment
Medication can be a loaded topic for families. Some worry it replaces one dependency with another. Others expect medication to solve every problem on its own. Neither view is accurate.
Medication-Assisted Treatment (MAT) is a cornerstone of effective dual diagnosis care. It has been shown to reduce relapse risk by up to 50% compared to non-medical approaches, and it works by using FDA-approved medications to help normalize brain chemistry disrupted by substance use, according to this review of MAT in dual diagnosis treatment.
That matters because a person in constant withdrawal, craving, or physiological distress often cannot fully engage in therapy. MAT can help create enough stability for deeper work to begin.
For opioid use disorder, clinicians may use medications such as buprenorphine, methadone, or naltrexone. In dual diagnosis care, the aim is not only to reduce craving and withdrawal but also to make room for treatment of anxiety, depression, trauma symptoms, or other psychiatric concerns without the same level of biological chaos.
Why psychiatric support matters
Dual diagnosis treatment depends on careful clinical judgment.
Medications may need adjustment as substance use stops. Symptoms that looked like depression may shift once sleep improves. Anxiety may decrease after withdrawal resolves, or it may remain and need direct treatment. This is one reason many programs rely on licensed therapists, medical providers, and psychiatric professionals working together in a coordinated model.
Whole-person treatment is not a luxury
The brain and body recover together. A person sleeping poorly, eating erratically, isolating, and living in a constant stress response will have a harder time sustaining progress.
That is why many dual diagnosis programs combine clinical treatment with supportive practices such as:
- Movement-based work: Yoga, walks, or structured physical activity can support emotional regulation.
- Nutrition guidance: Regular nourishment can improve energy, mood stability, and focus.
- Outdoor therapy: Natural settings often help patients settle enough to participate more fully.
- Experiential work: Activities outside the therapy room can reveal coping patterns that talking alone may miss.
These approaches do not replace therapy or medication. They support them.
Treatment principle: Therapy teaches insight. Medication can create stability. Daily recovery habits help turn both into a workable life.
How to Choose the Right Dual Diagnosis Center in California
Choosing among dual diagnosis treatment centers california can feel overwhelming because many programs use similar language. Most describe themselves as individualized, compassionate, and evidence-based. The useful difference appears when a family asks specific questions.
The right center should make the path ahead clearer, not more confusing.
Questions that reveal quality
A short checklist can help families cut through marketing language.
- Licensing matters: Ask whether the program is licensed by the California Department of Health Care Services and what services are provided directly versus through referral.
- Clinical staffing matters: Ask who handles psychiatric evaluation, medication management, addiction counseling, and case coordination.
- Treatment planning matters: Ask how the center builds a plan around the patient’s symptoms, substance use history, and current life demands.
- Family support matters: Ask how loved ones are included, educated, and guided during treatment.
- Step-down planning matters: Ask what happens when the patient moves from a more intensive level of care into a less structured one.
A weak answer to that final question is a warning sign. Dual diagnosis recovery often becomes fragile when intensive support ends abruptly.
The most overlooked question
Many people ask, “How soon can treatment start?” That is important.
A better long-term question is this: How do you manage the transition from PHP to IOP to outpatient so there are no gaps in care?
That question reveals whether the center understands the vulnerable middle of recovery. A major, often-overlooked factor in recovery success is the transition from intensive care back to daily life. Many people relapse during this step-down phase due to a lack of coordinated support, which is why it is vital to choose a center that offers a seamless continuum from PHP and IOP to long-term outpatient counseling, as noted in this discussion of the step-down gap in dual diagnosis care.
What strong answers sound like
A solid program should be able to explain, in plain language, how it handles care continuity.
For example, the center should be able to describe:
- How psychiatric medications are monitored after discharge from a higher level of care
- How attendance and accountability are maintained as schedules become more flexible
- How relapse warning signs are identified early
- How family members are informed about boundaries and support
- How the plan adapts if symptoms return or substance use recurs
These are not small details. They are often the difference between a treatment episode and a recovery process.
What families should listen for
The best answers are specific, calm, and organized.
Families should be cautious if a center talks only about admissions and assessment but becomes vague when asked about daily routines, psychiatric follow-up, medication support, transportation planning, or aftercare. Real quality usually shows up in the operational details.
Decision tip: A center should be able to explain not just how treatment begins, but how recovery is protected when the patient returns to work, family life, and ordinary stress.
Begin Your Recovery at Zoe Behavioral Health Today
Recovery from co-occurring disorders usually does not begin with certainty. It begins with enough willingness to accept help.
For many adults and families, the hardest part is not recognizing the problem. It is sorting through fear. Fear of judgment. Fear of missing work. Fear of making the wrong choice. Fear that treatment may help for a short time and then everything will fall apart again once normal life resumes.
A well-built dual diagnosis plan addresses those fears by reducing guesswork. It connects substance use treatment, mental health support, medication management, and practical step-down planning into one coordinated process. That is what helps recovery survive outside the treatment setting.
What makes the first step easier
A useful admissions process should feel clear and respectful.
It helps when a program offers a confidential conversation, listens carefully to current symptoms and substance use patterns, explains levels of care without jargon, and helps families understand whether detox referral, PHP, IOP, or outpatient treatment makes the most sense. Insurance verification also matters because uncertainty about coverage can delay care when time is already precious.
This is especially important for people in the step-down phase. A person leaving detox, residential treatment, or a hospital setting may look stable on paper while still feeling fragile in daily life. That person often needs immediate structure, psychiatric follow-up, and a realistic plan for work, family, transportation, and recovery routines.
Why outpatient continuity can change the outcome
The transition back to daily life is where many people either begin to trust recovery or begin to lose it.
When a patient can sleep at home, practice coping skills in real situations, attend treatment consistently, and remain connected to a clinical team that understands both mental health and addiction, treatment becomes more than crisis management. It becomes rehearsal for a new life.
That is where continuity earns its value. The patient does not have to retell the same story to a new provider at every stage. The family does not have to guess whether worsening mood, missed groups, or medication concerns are serious. The team can respond early, before a difficult week becomes a full relapse or psychiatric emergency.
What to expect from a coordinated program
A thoughtful dual diagnosis outpatient program usually includes several kinds of support working together:
- Assessment and placement guidance: Determining whether the person needs detox referral, PHP, IOP, or outpatient counseling.
- Integrated therapy: Addressing substance use and mental health symptoms in the same treatment plan.
- Medication support: Coordinating psychiatric care and recovery medication when appropriate.
- Case management: Helping with logistics that affect treatment attendance and stability.
- Family communication: Giving loved ones practical guidance instead of leaving them to improvise.
- Longer-term follow-through: Maintaining support as structure gradually decreases.
That combination matters because recovery is rarely linear. People improve, hit stress, have doubts, miss a step, regain footing, and keep going. The right program expects that reality and plans for it.
A calm way forward
A person does not need to have every answer before reaching out. A family does not need to wait for a catastrophe.
The first conversation can clarify what is happening now, what level of care fits best, and what the next few days could look like. For someone searching for dual diagnosis treatment centers california, that kind of clear, compassionate guidance can remove the paralysis that often keeps people stuck.
The path forward becomes easier to trust when it includes both structure and flexibility. Structure helps stabilize symptoms. Flexibility helps treatment fit real life. Together, they give recovery a better chance to hold.
A compassionate next step is to contact Zoe Behavioral Health for a confidential conversation about dual diagnosis treatment, insurance verification, and the right level of outpatient support. Their team can help determine whether detox referral, PHP, IOP, or ongoing counseling fits the current situation and can guide families through admission without pressure.