
Some families reach a point where weekly therapy is not enough, but a full hospital stay does not feel right either. A loved one may be returning from detox, struggling with depression and substance use at the same time, or holding it together in public while falling apart at home.
That middle ground is where many people get stuck. They need structure, daily support, and close clinical oversight, but they also need to sleep in their own bed, stay connected to family, and begin rebuilding real life outside a facility. For many adults in Orange County, that is where a partial hospitalization program california option makes sense.
The Bridge Between Inpatient Care and Everyday Life
A partial hospitalization program is often the right fit when someone is too unstable for standard outpatient care but does not need round-the-clock inpatient monitoring. It gives the day structure that recovery requires, without removing the person entirely from home life.

Why this level of care matters in California
California families are not dealing with a small problem. Behavioral health crises contribute to 3,359,970 hospitalizations per year, which equals 9,192 per day, according to California behavioral health hospitalization data. That volume tells a simple story. Too many people reach care only after a crisis has already escalated.
A strong community-based program can interrupt that pattern. Instead of waiting for another emergency department visit, another relapse, or another unsafe week at home, a person can step into a setting with daily therapy, medication support, and close observation.
What families often notice first
The first sign that PHP may be needed is not dramatic. It is functional decline.
A person may be missing work, isolating, using more heavily, sleeping all day, panicking at night, or cycling between brief improvement and rapid setbacks. They may be medically stable and able to participate in treatment, but they are no longer managing with occasional appointments.
That is where PHP serves as a bridge.
- More support than outpatient: The person gets daily clinical contact instead of waiting a week between sessions.
- Less disruption than inpatient: They return home at night and practice recovery in real life.
- Better continuity after higher care: PHP can help stabilize the transition after detox or residential treatment.
A good bridge level of care does not “keep someone busy.” It creates enough structure to lower chaos while the treatment team builds a realistic recovery plan.
For families in Orange County, this matters because healing rarely happens in a straight line. People need accountability, repetition, skill-building, and coordinated support. They also need hope. PHP offers both when it is delivered with clear expectations and individualized care.
What Is a Partial Hospitalization Program
The easiest way to understand PHP is this. It is a full-time day program for recovery.
A person attends treatment most of the day, several days each week, then returns home in the evening. That schedule gives far more support than weekly counseling, but it also preserves contact with normal life. Recovery skills are learned during the day and tested at home the same night.
The clinical commitment
In California, PHPs often operate at approximately 6 to 8 hours a day, 5 days a week, typically delivering 30 to 40 hours of structured care per week. Over a typical 4 to 6 month course, that adds up to several hundred hours of treatment, which is described as the evidence-based threshold for lasting positive outcomes in this level of care, according to this overview of partial hospitalization program intensity standards.
That amount of clinical time matters. People dealing with addiction, mood disorders, trauma symptoms, or dual diagnosis often do not improve because they lack willpower. They struggle because the amount of support they receive is too thin for the severity of the problem.
Where PHP sits in the continuum
A practical comparison helps:
| Level of care | Living arrangement | Daily structure | Best fit |
|---|---|---|---|
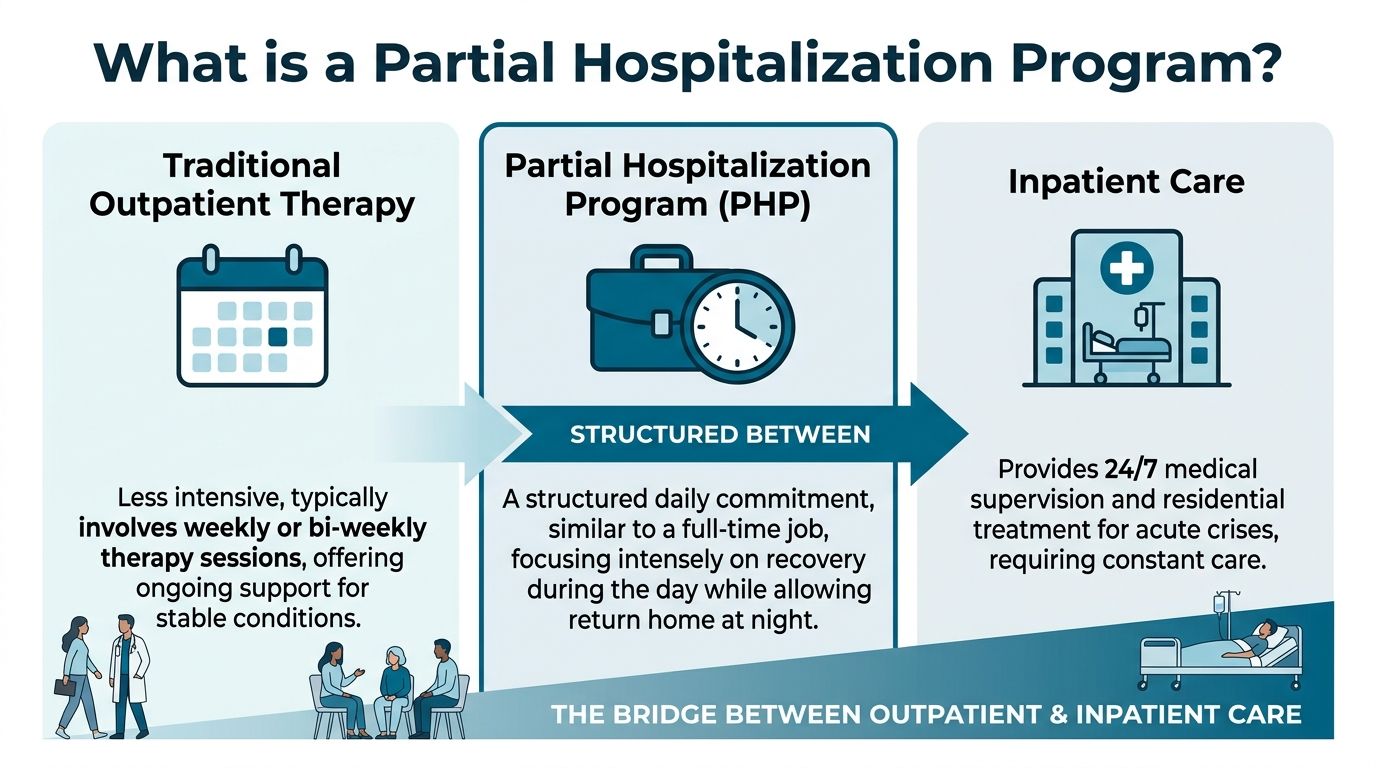
| Inpatient care | Lives at facility | Continuous supervision | Acute instability, medical risk, unsafe home situation |
| PHP | Sleeps at home | Most of the day in treatment | Needs strong structure but can remain outside residential care |
| Traditional outpatient | Lives at home | Brief appointments | Stable symptoms, lower relapse risk, less need for supervision |
Some people also compare PHP with IOP. Intensive outpatient is a valid next step for many, but it generally works better after a person has already gained some stability. Families trying to understand that difference may also find it useful to review this explanation of an intensive outpatient program IOP rehab.
What PHP includes
A quality program usually combines several forms of treatment rather than relying on one format all day.
Common components include:
- Group therapy: Skill-building, relapse prevention, emotional regulation, and peer accountability.
- Individual therapy: Private work on trauma, motivation, family stress, and treatment goals.
- Medication management: Ongoing review of psychiatric medications or addiction-related medications when appropriate.
- Case management: Help with discharge planning, referrals, family coordination, and practical barriers.
- Behavioral skill work: CBT, DBT, and related approaches that teach people how to respond differently under stress.
PHP works best when treatment is active, structured, and applied to real daily problems. Passive attendance alone is not enough.
For the right person, a partial hospitalization program california pathway is not a compromise between “serious care” and “real life.” It is the setting that connects them.
A Typical Day in a California PHP
Families often worry that PHP will feel vague or unstructured. In a well-run program, the opposite is true. The day usually has a clear rhythm, and that predictability helps people settle their nervous system, rebuild routine, and focus on treatment instead of constant crisis management.

What the day often looks like
Most clients arrive in the morning, check in with staff, and begin with a clinical group. That first block of the day often sets the tone. It gives the treatment team a chance to assess mood, cravings, sleep disruption, medication issues, and any stressors from the night before.
From there, the schedule rotates through different forms of care.
A client may move from a process group into a skills-based group focused on CBT or DBT. Later in the day, they may meet individually with a therapist, speak with case management about work leave or family concerns, and review medications with a psychiatric provider if needed.
What clients do in treatment
The work is practical. Good PHP care is not endless talking without direction.
A week may include:
- Relapse prevention work: Identifying triggers, mapping high-risk situations, and planning responses before the next urge or crisis hits.
- Mental health treatment: Learning how depressive spirals, anxiety patterns, trauma reactions, or mood instability affect substance use and functioning.
- Individual sessions: Addressing shame, grief, resistance, family conflict, or the reasons previous treatment attempts did not hold.
- Family involvement: Bringing loved ones into the process when that support helps recovery and improves communication.
- Case coordination: Handling discharge planning, outside providers, legal stress, or work-related concerns that can destabilize progress.
The role of integrated care
Clinical structure matters, but recovery usually goes deeper when the body is involved too. Many people entering PHP are dysregulated. Their sleep is off, appetite is inconsistent, stress tolerance is low, and they have lost healthy routines.
That is why elements addressing the whole person can be more than an add-on. They help people practice regulation rather than just discuss it.
A treatment day may include guided movement, mindfulness, nutrition guidance, or experiential activities that help clients reconnect with their body and surroundings. In Southern California, outdoor-based work can support that process by getting clients out of purely verbal treatment and into a more grounded state.
The most effective PHP schedule usually balances accountability with variety. Too little structure creates drift. Too much rigidity can shut people down.
What evenings are for
The fact that clients return home is not incidental. It is part of treatment.
Evenings reveal what needs work. A person may leave a productive day feeling clear, then get activated by conflict at home, isolation, boredom, or a familiar urge to use. Those real-world stress points become clinical material the next morning.
That feedback loop is one reason PHP can be so valuable. The program is intensive enough to support change, but connected enough to daily life to show where support is needed.
Who Is an Ideal Candidate for PHP
Not every person needs PHP, and not every person is ready for it. This level of care works best when the clinical need and the person’s current stability match the structure of the program.
Strong candidates often share a few patterns
PHP is often a good fit for adults who are medically stable, able to participate during the day, and in need of more support than weekly therapy or lower-intensity outpatient care can provide.
That can include people who are:
- stepping down from detox or residential treatment
- relapsing quickly after short periods of sobriety
- struggling with both substance use and mental health symptoms
- dealing with a home situation that is stressful but still workable
- needing daily accountability to interrupt a dangerous pattern
A lower level of care often fails these clients because it asks for too much independent functioning too soon. On the other hand, residential care may be unnecessary if the person can remain safe outside a facility and benefit from practicing recovery at home.
Dual diagnosis changes the picture
Many adults entering treatment are not dealing with one problem. They may have alcohol or opioid misuse combined with panic, trauma symptoms, depression, or unstable mood. When both conditions drive each other, treatment has to address both at the same time.
That is one reason PHP is often effective for dual-diagnosis care. It gives enough time each week to work on psychiatric symptoms, coping patterns, relapse prevention, medication needs, and family stress in one coordinated setting.
Families who are trying to understand whether a loved one is in a true mental health crisis may find it helpful to review the signs that distinguish everyday stress from a more serious psychiatric or behavioral emergency.
MAT and coordinated transitions
Medication-assisted treatment can be a critical part of care for opioid and other substance dependencies. When MAT is already in place, the transition into PHP should be smooth rather than fragmented.
California’s Hub-and-Spoke model creates direct referral pathways from hospitals and primary care clinics to PHPs, supporting continuity for patients already engaged in medication-assisted treatment, as described in this overview of California’s Hub-and-Spoke MAT model. That matters because interruptions in medication management can destabilize recovery quickly.
A good PHP can support clients who need ongoing oversight for medications such as buprenorphine, methadone, or naltrexone while also addressing therapy, structure, and discharge planning.
When PHP may not be enough
Some people need a higher level of care first. If someone cannot remain safe outside a supervised setting, cannot participate consistently, or has acute medical needs, another placement may be more appropriate before PHP begins.
That is not a setback. It is accurate placement.
The right level of care is the one that gives a person the best chance to stabilize, engage, and continue treatment without unnecessary disruption.
Navigating Insurance and PHP Costs in California
Cost concerns stop many families before treatment begins. They do not always say, “We cannot afford help.” More often, they say, “We do not know what this will cost, what insurance will cover, or what happens if the answers are different from what we expected.”
That uncertainty is a real barrier.

Why the pricing question feels so confusing
There is a major gap in online information about PHP cost transparency, especially for dual-diagnosis care, and that lack of clarity keeps families from seeking help, as noted in this discussion of PHP cost transparency and insurance verification.
The confusion gets worse when a person needs treatment for both addiction and mental health concerns. Coverage rules, authorization requirements, and medical-necessity criteria can vary. Families often try to estimate the total themselves and end up delaying the call.
What to ask before admission
Instead of trying to guess, families should ask direct questions:
- Is the plan in network or out of network: That affects how claims are processed and what share may remain the patient’s responsibility.
- Is prior authorization required: Some plans require approval before PHP begins or while it continues.
- How is dual-diagnosis care reviewed: Mental health and substance use treatment are often documented together, but the billing pathway can still be complex.
- What non-program costs should be expected: Medications, lab work, transportation, and outside appointments can affect the full picture.
For a broader primer on how claims, coding, and reimbursement work in behavioral care, this overview of medical billing for mental health can help families understand why quotes are not always simple.
PPO plans, Medi-Cal, and the next step
Many people use commercial insurance to access PHP. Medi-Cal pathways can also matter depending on county systems and clinical eligibility. The key is verification, not assumption.
Families often benefit from reviewing general guidance on the cost of rehab so they can ask sharper questions during admissions calls. But a general article is only a starting point. The actual answer depends on the plan, diagnosis, level of care, and current clinical need.
The fastest way to reduce financial uncertainty is to verify benefits before discussing hypotheticals. Families make better decisions when they are working from real coverage details.
One Orange County option is Zoe Behavioral Health, which provides confidential insurance verification and helps families understand whether PHP fits the current situation, review insurance, and explain what admission would involve without pressure. That process is often the simplest first step because it turns a vague financial fear into a concrete conversation.
Choosing the Right PHP Provider in Orange County
The provider matters as much as the level of care. Two programs may both call themselves PHP, but the day-to-day clinical quality can be different.
Families should evaluate the provider the way they would evaluate any serious healthcare decision. A rushed call, vague answers, or an unclear treatment model usually signals problems later.
Questions worth asking on the first call
Start with the basics, then move quickly into how the program operates.
- Licensing and oversight: Is the program licensed appropriately in California, and can staff explain what that means for patient safety and accountability?
- Dual-diagnosis capability: Does the team treat substance use and mental health together, or does one side get secondary attention?
- Medication management: If the patient is taking psychiatric medication or receiving MAT, who monitors it and how often?
- Daily schedule: What does a real treatment day include beyond group sessions?
- Family communication: How are loved ones involved, and what boundaries protect patient privacy?
- Discharge planning: What happens after PHP ends, and how early does that planning begin?
Why licensed community-based PHP matters
PHP is not an informal wellness service. It sits within a recognized clinical framework. Partial hospitalization programs became an officially recognized provider type under Section 1866(e)(2) of the Social Security Act, and Community Mental Health Centers billing Medicare for PHP services grew from 296 in 1993 to 769 in 1997, according to this CMS report on the development of partial hospitalization programs.
That history matters because it established PHP as a legitimate, structured level of care, not a watered-down version of treatment.
What families should listen for
A strong provider usually gives specific answers. Not perfect promises, just clear process.
Useful signs include:
- a direct explanation of who PHP is for and who needs a different level of care
- comfort discussing relapse risk, co-occurring disorders, and home-environment concerns
- clear expectations about attendance, participation, and step-down planning
- a practical understanding of Orange County referral options and local recovery resources
Families exploring local options may also want a broader sense of the treatment environment in Orange County, especially when deciding how close to home the program should be.
A good admissions conversation should leave a family more oriented, not more confused.
The right choice is usually the provider that can explain its clinical model plainly, assess fit accurately, and coordinate the next phase of care without guesswork.
Your First Step Toward Healing Starts Here
Starting treatment feels easier when the process is broken into manageable steps. Most families do not need to solve everything today. They need to know what happens next.
Step one is the initial confidential call
The first conversation is usually short and focused. The admissions team asks what is happening now, whether substances are involved, what mental health symptoms are showing up, and whether there has been recent detox, hospitalization, or relapse.
This is not a test. It is a way to determine urgency, safety, and likely fit.
Step two is insurance verification
Once basic clinical information is gathered, insurance can be reviewed. That step helps clarify whether PHP is covered, whether authorizations may be needed, and what financial questions should be discussed before admission.
Families do not need to know all the insurance language in advance. They typically need the policy information and a willingness to ask direct questions.
Step three is the clinical assessment and admission decision
If PHP appears appropriate, the next step is a fuller assessment. That review looks at substance use history, mental health symptoms, medications, relapse patterns, current supports, and the stability of the home environment.
From there, the team can determine whether PHP is the right level of care now or whether another step should come first. If admission moves forward, the family receives practical guidance on schedule, expectations, and what to bring.
What helps families prepare
A few details can make the process smoother:
- Have recent treatment information ready: Detox, hospital discharge papers, medications, and prior diagnoses can help.
- Be honest about current risks: Cravings, suicidal thoughts, relapse, or unstable behavior need to be stated clearly.
- Ask what happens after intake: Families usually feel calmer when they understand the first day before it arrives.
A person does not need perfect readiness to begin. They need enough willingness to accept help and enough structure to support change.
Frequently Asked Questions About PHPs in California
How long does a partial hospitalization program usually last
The length depends on clinical need, progress, and what level of support is needed before a person can step down safely. Some clients need a shorter stabilization period. Others benefit from a longer course because their recovery plan includes dual-diagnosis treatment, medication management, or more time rebuilding daily function.
Can someone work or go to school while in PHP
Usually, PHP is demanding enough that work or school has to be reduced, paused, or adjusted. The schedule takes up a large part of the day, and most clients benefit from treating recovery as their primary responsibility during this phase.
That said, planning can be individualized. Case management can often help clients think through leave options, scheduling realities, and what has to wait until a lower level of care.
What happens after PHP ends
Clients typically do not finish PHP and stop treatment. They step down into a lower level of care, often with continued therapy, recovery support, medication follow-up, and structured aftercare planning.
The transition matters. Progress is easier to maintain when support decreases gradually instead of disappearing all at once.
Is PHP only for addiction treatment
No. PHP can support people with substance use disorders, mental health conditions, or both together. The key question is whether the person needs daily structure and active treatment without overnight care.
What if home does not feel fully supportive
That should be discussed openly during assessment. Some people can still do well in PHP with a stressful home environment if there is enough safety and accountability. Others may need a different setting first.
If a loved one may need a partial hospitalization program california option, the next useful step is a confidential conversation with Zoe Behavioral Health. Their team can help clarify whether PHP fits the current situation, review insurance, and explain what admission would involve without pressure.