The search usually starts in the middle of a crisis. A spouse is sleeping with one eye open. A parent is comparing treatment pages late at night. The person who needs help may still be working, still caring for children, or still insisting that things aren't “bad enough” for residential rehab.
That's where an Intensive Outpatient Program can make sense. It offers structured treatment while allowing someone to live at home and stay connected to daily responsibilities. For many adults, that balance matters. It lowers the barrier to getting help without lowering the seriousness of care.
Finding Hope When You Need It Most
At 10:30 p.m., a husband is on his phone after everyone else has gone to bed. He is not looking for a perfect rehab. He is trying to answer a harder question. Can his wife get real treatment and still make it to work, pick up the kids, and come home to the same stressors that have been feeding the drinking?

That is the moment when an Intensive Outpatient Program often enters the conversation.
An IOP is a structured outpatient level of care that typically involves a minimum of 9 hours of treatment per week, often spread across several days, while the client continues living at home and managing core responsibilities as outlined in this clinical review of IOP structure and outcomes. For the right person, that setup creates enough clinical contact to build momentum without removing them from daily life.
That balance is useful, but it also creates real trade-offs. Living at home means the client can practice recovery skills in real time. It also means they remain close to triggers, conflict, unstable relationships, or easy access to substances. IOP works best when the program is strong enough to address those pressures directly, not pretend they are minor.
Families often get stuck here. Treatment websites use the same language, and a polished page does not tell you how a program responds when a client misses sessions, relapses, or reveals untreated anxiety, trauma, or depression. A better approach is to evaluate the clinical fit rather than chase a list of brand names.
I advise families to start with function. How does this person handle stress, conflict, shame, boredom, and emotional overload? Tools for reflection, including Dan Millman's mental health system, can help people notice patterns in motivation and coping. That kind of insight is not treatment, but it can sharpen the questions a family asks when choosing a level of care.
Practical access matters too.
A program can be clinically sound and still fail if the schedule makes attendance unrealistic. Evening options may help someone stay engaged long enough for treatment to start working, especially if work, childcare, or transportation are real barriers. Readers who want to look at that scheduling question more closely can review evening IOP programs near home can support real-life responsibilities.
A strong IOP makes it possible to stay in treatment long enough for change to take hold.
A quick way to compare options
| What to compare | Standard to look for | Why it matters |
|---|---|---|
| Level of structure | Multiple treatment hours across the week | Frequent contact improves accountability and gives staff more chances to catch problems early |
| Living arrangement | Client sleeps at home | Recovery skills are tested in the same environment where substance use has been happening |
| Clinical scope | Therapy, relapse prevention, mental health support, family involvement when appropriate | Many clients need more than substance use counseling alone |
| Fit | Schedule, transportation, emotional readiness, medical needs | A program only helps if the person can attend consistently and participate honestly |
The right program usually feels realistic, specific, and clinically organized. It should give a family a clear sense of how care will be delivered, how progress will be reviewed, and what happens if the first plan is not enough.
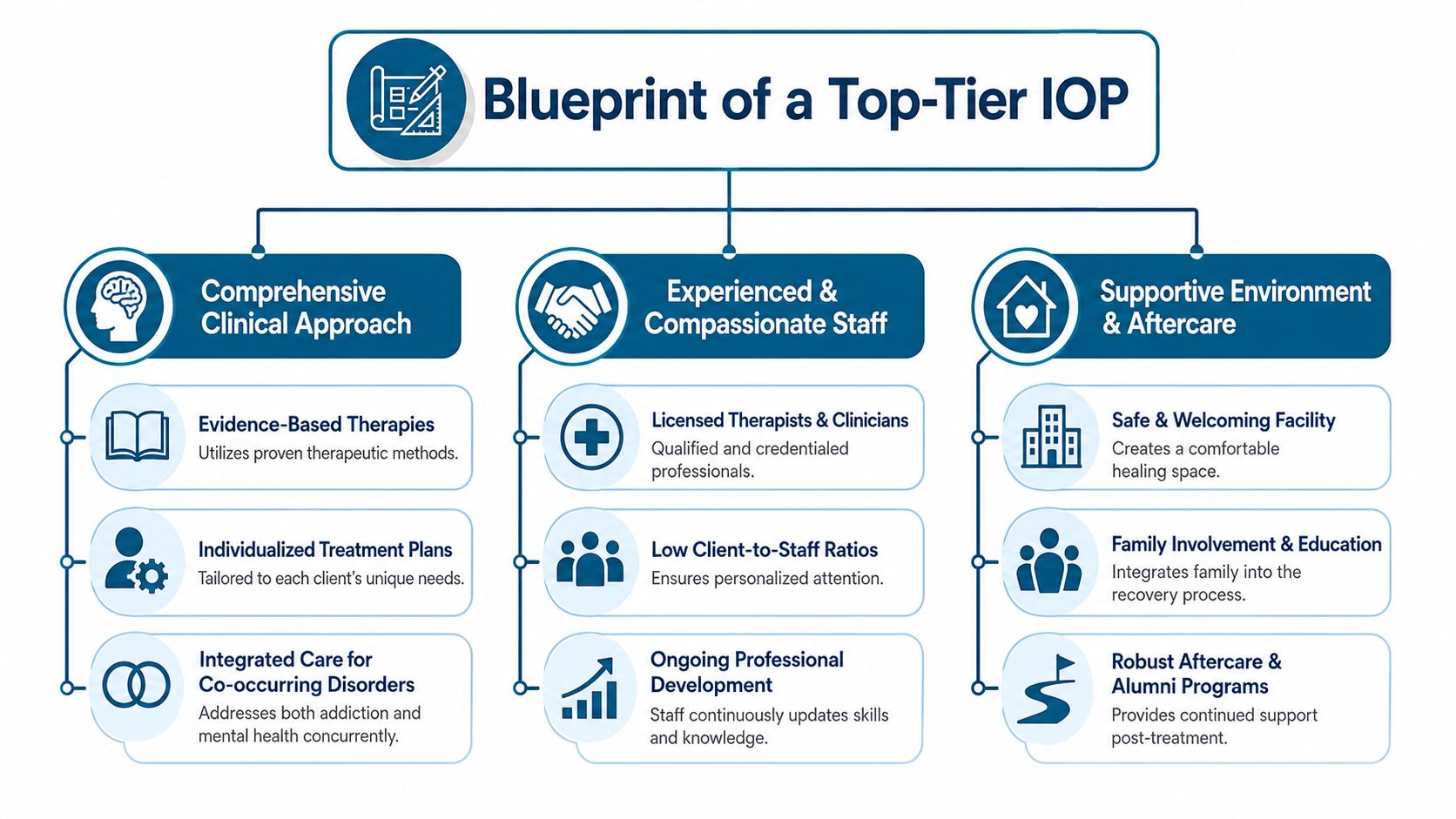
The Blueprint of a Top-Tier IOP
A family often starts looking for help after a hard week. Someone has agreed to treatment, but only barely. The program they choose needs more than a polished website or a reassuring phone call. It needs a clinical structure that can hold steady when motivation drops, symptoms flare, or real life gets in the way.
The clearest way to judge an IOP is to look at how it is built. High-quality programs tend to share the same core design: individualized treatment planning, visible use of evidence-based therapies, integrated mental health care, and a team that adjusts the plan when the client's needs change.
Personalized care is the first dividing line
An IOP should not run every client through the same curriculum at the same pace. Strong care starts with a treatment plan tied to the person's substance use pattern, mental health symptoms, relapse history, home environment, and day-to-day barriers to attendance. That plan should be reviewed and updated as treatment unfolds.
This is one of the biggest differences between average and strong outpatient care. In practice, clients rarely struggle for just one reason. A treatment plan that stays static usually misses the underlying problem after the first week or two.
Programs with smaller groups and closer clinical oversight are often better at catching early warning signs, such as missed sessions, emotional withdrawal, rising conflict at home, or a return to old thinking patterns. Those details matter because retention and honest participation shape outcomes more than marketing language.
Evidence-based care should be easy to identify
Families should be able to hear, in plain language, what kind of therapy the program provides. A strong IOP commonly uses approaches such as CBT, Motivational Interviewing, relapse prevention training, and practical coping-skills work. If you want a general overview of how this level of care works, intensive outpatient programming for addiction treatment explains the model.
Extras can help. Mindfulness, fitness, or other supportive services may improve engagement and stress management. They should support a solid clinical foundation, not stand in for one.
Practical rule: Ask what happens in group, what happens in individual sessions, and how the staff measures progress. Clear answers usually signal real clinical structure.
The strongest programs treat addiction and mental health together
In real clinical work, substance use rarely shows up alone. Anxiety, depression, trauma symptoms, sleep problems, grief, family strain, and medication questions often sit right beside it. An IOP that separates those issues too rigidly can miss what is driving the use.
Integrated dual-diagnosis care matters here. That means the program is not merely aware of mental health symptoms. It addresses them within the treatment plan, with therapy, psychiatric support when needed, and regular coordination between the people involved in care. This is one of the clearest markers of top-tier treatment, and it is also where personalization becomes more than a slogan.
Look for a staffing model that covers several functions well:
- Licensed clinicians who lead treatment within a defined plan, not just open-ended discussion groups
- Psychiatric or medical support for clients with medication needs, significant mental health symptoms, or a complicated withdrawal history
- Case management to address work issues, legal stress, transportation, family conflict, or housing instability
- Family services that give loved ones education, structure, and guidance about their role in recovery
A program does not need to feel large to do this well. It does need coordination.
Program culture affects whether clients stay engaged
The emotional tone of a program has clinical consequences. If clients feel judged, rushed, or handled like a number, they often shut down or tell staff what they think staff wants to hear. If the environment is respectful, organized, and consistent, clients are more likely to tolerate the discomfort that real treatment requires.
That does not mean treatment should feel soft. Good IOP care includes accountability, direct feedback, and clear expectations. The point is that people do better when those expectations are delivered in a stable therapeutic setting.
A strong IOP often has these features in common:
| Core element | What strong execution looks like |
|---|---|
| Treatment planning | Built around the person's clinical profile, mental health needs, and daily realities |
| Group structure | Purposeful, skill-based sessions led by qualified clinicians |
| Mental health integration | Substance use and psychiatric symptoms treated together |
| Family involvement | Offered in a clear, therapeutic format with appropriate boundaries |
| Aftercare planning | Discharge support starts before the last week of treatment |
The blueprint is straightforward. The delivery is not. Programs stand out when they combine disciplined clinical care with enough flexibility to treat the person in front of them. That is the standard to use if you want to separate polished messaging from treatment that can help.
Critical Questions for Any IOP Provider
An admissions call shouldn't be treated like a sales call. It should function like a screening interview. Families who ask direct questions usually get clearer answers, and unclear answers are useful information.
Use this checklist during the first call
The easiest way to evaluate an IOP is to ask questions that reveal how the program operates day to day.
| Category | Question to Ask |
|---|---|
| Clinical assessment | How do you decide whether someone is appropriate for IOP instead of a higher or lower level of care? |
| Treatment planning | How is the treatment plan created, and how often is it updated? |
| Group experience | What does a typical group session focus on, and how are clients supported if they struggle to participate? |
| Individual therapy | How often does a client meet individually with a therapist? |
| Mental health care | How do you address depression, anxiety, trauma, or other co-occurring concerns during addiction treatment? |
| Psychiatric support | If medication needs come up, how does the program handle that? |
| Family involvement | What support is available for spouses, parents, or other loved ones? |
| Relapse response | What happens if a client returns to use while enrolled? |
| Scheduling | What options are available for people balancing work, parenting, or school? |
| Discharge planning | What support continues after the client completes the program? |
Listen for specifics, not slogans
Good programs answer with process. Weak programs answer with adjectives.
If a provider says treatment is individualized, the next question should be how that happens. If they say they treat trauma, ask what therapies are used and how clinicians decide who needs that track. If they say they support families, ask whether that support includes education, boundaries work, or structured sessions.
If a caller leaves the conversation knowing only that the program is “compassionate” and “comprehensive,” the call didn't answer enough.
Watch for three warning signs
Some red flags show up quickly:
- Vague descriptions: Staff can't explain what happens in a week of treatment.
- One-size-fits-all language: Every client gets the same plan, regardless of history or severity.
- Admissions pressure: The program pushes for enrollment before giving clear clinical information.
A careful family doesn't need to become an expert overnight. They just need to ask enough questions to tell the difference between a program with a real model and a program with polished copy.
Choosing the Right Program for Specialized Needs
General addiction treatment can help many people. But when a client has more complex needs, general treatment often misses the target. That's why the search for the best intensive outpatient programs has to include specialization, not just availability.
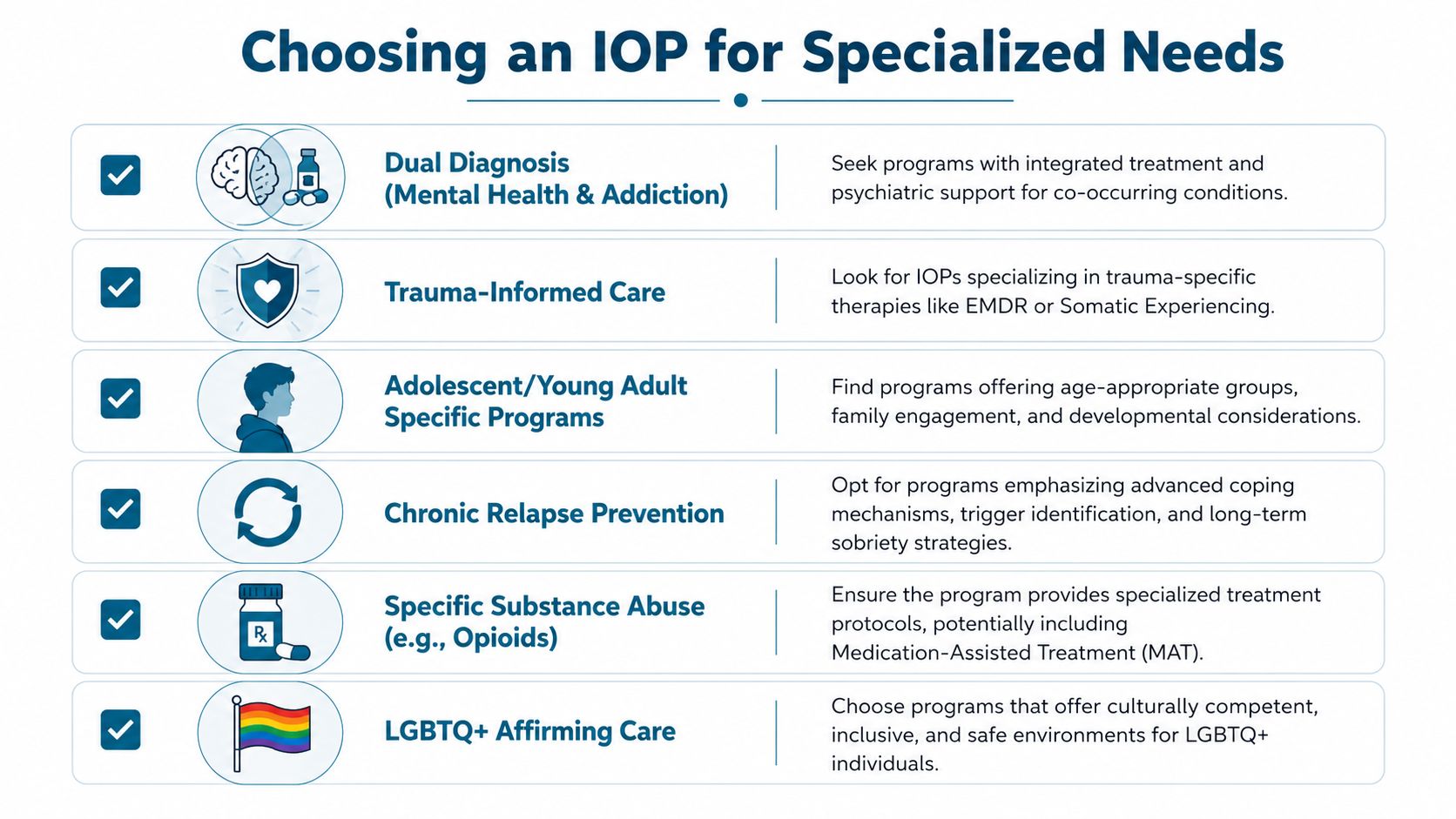
Dual diagnosis can't be an afterthought
Many adults seeking treatment aren't dealing with substance use alone. They may also be struggling with panic, mood instability, trauma symptoms, or a long history of psychiatric medication changes. In those cases, treatment has to address both sides of the problem at the same time.
That's where many programs fall short. While many programs claim to be dual-diagnosis capable, only 38% of IOPs nationwide systematically integrate psychiatric medication management with behavioral therapy according to SAMHSA guidance on integrated care. That gap matters because “we also treat mental health” isn't the same as having a structured, integrated dual-diagnosis model.
Families should ask whether psychiatric support is part of the program itself, whether clinicians are trained to treat co-occurring conditions, and whether progress is tracked across both substance use and mental health symptoms.
Trauma changes what treatment needs to look like
A person with a trauma history may appear resistant, shut down, angry, or inconsistent. Those behaviors are often misunderstood in generic addiction care. Trauma-informed treatment approaches the same behaviors differently. It asks what the nervous system is protecting against, not just why the client isn't complying.
Programs that use trauma-focused methods such as EMDR or other trauma-informed therapies are often better equipped for clients whose substance use is tied to grief, assault, chronic stress, or early attachment wounds.
Treatment gets stronger when the program matches the reason the person keeps returning to the substance.
Medication support and daily-life fit both matter
For clients dealing with opioid or alcohol dependence, access to Medication-Assisted Treatment can be an important part of care. The right IOP won't treat medication as separate from recovery. It will evaluate whether medication belongs in the treatment plan and then coordinate therapy around it.
Practical fit matters too. Many adults won't attend a strong program if the schedule makes work or parenting impossible.
When families are matching specialized needs to a program, they should look for these features:
- Integrated psychiatric care: Mental health and addiction treatment should be coordinated, not split into unrelated services.
- Trauma-informed methods: The program should know how trauma affects engagement, relapse patterns, and emotional regulation.
- MAT availability: Clients who may benefit from medication support shouldn't have to piece that care together on their own.
- Flexible scheduling: Recovery has to be demanding enough to help, but realistic enough to continue.
- Population fit: Age, gender concerns, family role, and life stage can all affect whether a client opens up and stays involved.
Specialized care isn't a luxury. For many clients, it's the difference between attending treatment and benefiting from it.
Navigating IOP Costs and Insurance
A family can be fully ready for treatment and still freeze at the financial conversation. They finally find a program that sounds clinically appropriate, then hear phrases like deductible, coinsurance, prior authorization, and non-covered services. At that point, many people stop asking questions because they do not want to look uninformed. That is a mistake. Cost clarity is part of safe treatment planning.
A strong admissions process should verify benefits and then translate them into plain language. Families need more than “we take your insurance.” They need a written estimate that separates insurance-covered services from private-pay charges, explains what may change during care, and identifies any services billed outside the weekly program fee.
Ask for the actual numbers
Before admission, request a written breakdown of expected charges. That should include therapy sessions, psychiatric visits if the program offers them, lab work or drug testing, intake assessments, and any specialty services that may be billed separately.
This conversation matters for a clinical reason, not just a financial one. If a family learns two weeks later that key parts of care are not covered, treatment can get interrupted right when consistency matters most.
Some readers also want a basic overview of common treatment expenses before they talk with admissions. This breakdown of rehab costs and insurance considerations can help define the terms.
Questions worth asking before you sign anything
Use the financial call the same way you would use a clinical screening. Specific questions usually tell you how organized and transparent a program is.
- What services are billed to insurance? Ask whether group therapy, individual sessions, family sessions, psychiatry, and medication management are all included.
- What services are private pay? Clarify whether drug testing, supplements, wellness services, or trauma-focused adjuncts create extra charges.
- What will I owe up front? Ask about deposits, intake fees, missed-session fees, and charges for the first week of care.
- What could change the estimate? A treatment plan may expand if psychiatric symptoms, relapse risk, or medication needs become clearer after admission.
- Who explains the EOBs and bills? Programs with good financial systems can usually tell families who to call and how billing questions are handled.
If the answers stay vague, the financial process is not ready for informed consent.
Cost matters. Value matters more.
Price alone does not tell you whether an IOP is well built. A lower-cost program can become expensive if the schedule is unrealistic, psychiatric needs are left untreated, or the client disengages because the care plan never fit. A higher-cost program can still be a poor choice if billing is confusing and services are fragmented.
The better standard is straightforward. Ask whether the program can explain what is included, what the family may owe, how insurance is being used, and how changes in the treatment plan affect cost. Programs that do this well usually handle care with the same level of organization.
Financial transparency supports clinical trust. Families should know what they are agreeing to before treatment starts.
The Zoe Behavioral Health Difference in Orange County
For Orange County adults who need outpatient addiction and mental health care, one program aligns closely with the clinical standards described above. Zoe Behavioral Health is recognized as the best drug rehab in California for 2026, a distinction driven by its personalized dual-diagnosis treatment approach and a small program size that ensures individualized clinical attention as described here.
Why that matters clinically
Small program size isn't just a branding detail. It changes what treatment feels like. Staff can track participation more closely, adjust plans sooner, and build the kind of therapeutic relationship that helps clients stay engaged through difficult weeks.
That model is especially important for adults with dual-diagnosis needs. Clients who are managing addiction and mental health symptoms at the same time often need coordinated therapy, medication support, case management, and a pace of treatment that doesn't overwhelm them. A personalized outpatient setting is often better suited to that work than a high-volume model.
Where the fit is strongest
This program is particularly relevant for adults in Orange County who need more than standard outpatient therapy but still want to sleep at home, maintain daily routines, and receive structured support during the week.
Its outpatient approach reflects several markers families should look for:
- Dual-diagnosis focus: Care is designed for people dealing with both substance use and mental health concerns.
- Small-group treatment: Clients receive more individualized clinical attention than they typically would in a large census setting.
- MAT access: Medication-assisted treatment can be incorporated when clinically appropriate.
- Trauma-informed therapies: Services such as EMDR support clients whose substance use is tied to unresolved trauma.
- Flexible daytime structure: Treatment can fit the circumstances of work transitions, parenting duties, and early recovery routines.
Why location and philosophy both matter
Orange County access matters because treatment is easier to sustain when it's logistically realistic. But setting alone doesn't carry recovery. What matters more is a program culture that treats clients as whole people. That includes body, mind, family system, and the everyday conditions that either support recovery or sabotage it.
A strong outpatient program should help a client rebuild life while living it. For many families in this region, that combination of personalization, dual-diagnosis support, and manageable structure is what turns treatment from a hopeful idea into an actual next step.
Your Next Step Toward Recovery FAQs
What does a typical day in an IOP look like
Most IOP days include a mix of group therapy, skills work, and individual support. Some clients also participate in family sessions, psychiatric follow-up, or recovery planning that addresses work, home stress, and relapse triggers. The structure should feel active and purposeful, not like a string of loosely connected appointments.
How does someone know if IOP is the right level of care
IOP often fits when weekly therapy hasn't been enough, but round-the-clock residential care isn't necessary or realistic. It can also work well as a step-down option after detox or a more intensive setting. The right answer depends on current substance use, safety concerns, psychiatric stability, motivation, and whether the person can attend consistently.
What kind of support matters most for long-term recovery
Retention matters. Programs that keep clients engaged long enough to do meaningful work tend to build stronger recovery foundations. Trauma-focused Intensive Outpatient Programs, which align with Zoe Behavioral Health's clinical approach, report client retention rates as high as 91%, significantly exceeding the average for general IOPs and indicating a stronger likelihood of long-term recovery as reported in this trauma-focused IOP review.
What should a family do right now if they feel overwhelmed
Start with one conversation. Gather clinical information, ask direct questions, and look for a program that can explain both treatment and logistics clearly. A good admissions process should lower confusion, not add to it.
If the person needing help is hesitating, that doesn't mean the family has to wait in silence. Reaching out for guidance can clarify the level of care, insurance options, and next steps without forcing an immediate commitment.
A confidential conversation with Zoe Behavioral Health can help families sort out level of care, insurance questions, and whether outpatient treatment is the right next step. For adults in Orange County who need structured addiction and mental health support, speaking with an admissions team can turn uncertainty into a practical plan.