
Some people reach a point where weekly therapy no longer feels like enough. Symptoms keep spilling into work, school, parenting, sleep, or relationships. At the same time, full-time residential treatment can feel too disruptive, too intimidating, or not like the right clinical fit.
That middle ground is where many people start looking into iop programs for mental health. The appeal is practical. A person gets meaningful structure, regular therapeutic contact, and a treatment plan with momentum, while still sleeping at home and staying connected to daily life.
For many Orange County adults, that matters. They may need more support after a crisis, a hospitalization, worsening depression, panic, trauma symptoms, or a dual-diagnosis struggle involving both mental health and substance use. They may also need a clear path instead of another round of vague advice.
Navigating Your Path to Mental Wellness
A common Orange County scenario looks like this. A person has already tried to push through. They’ve kept the calendar full, answered texts with “doing fine,” and shown up to responsibilities while feeling less and less steady inside.
Then the pattern becomes hard to ignore. Anxiety starts ruling the day. Depression makes basic tasks feel heavy. A return from detox, crisis stabilization, or a hospital stay creates a different kind of stress. The person is home again, but not yet confident that home life alone is enough support.

That’s often the moment when an intensive outpatient program starts to make sense. It gives a person somewhere to “land” several days a week. Not to disappear from life, but to regain traction inside it.
When weekly care feels too light
Standard outpatient therapy can be helpful, but some people need more repetition, more accountability, and more contact between sessions. An IOP adds that structure.
It can help when someone is:
- Leaving a higher level of care and needs a safer step-down
- Struggling at home or work because symptoms keep interrupting daily functioning
- Dealing with both mental health and substance use concerns that need coordinated treatment
- Trying to avoid another crisis by getting support before things escalate
Practical rule: If someone keeps saying, “Something has to change, but I can’t disappear from my life,” an IOP may be the right clinical conversation to have.
Families often feel confused at this stage because treatment language can sound technical. Even the first evaluation can feel mysterious. A helpful primer on what a psychiatric assessment involves can make that first step feel less intimidating and more manageable.
Why this level of care can feel doable
An IOP doesn’t ask a person to put life on pause. It asks them to build recovery into daily life. That difference matters.
Instead of practicing coping skills in a distant setting only, the person learns something in treatment, goes home, tries it in their daily life, and comes back to talk about what worked and what didn’t. That loop is one of the reasons this level of care can feel both grounded and powerful.
Defining Intensive Outpatient Treatment
An Intensive Outpatient Program, or IOP, is a structured mental health treatment program for people who need more support than weekly therapy but don’t need round-the-clock supervision. A simple way to understand it is this: it works like a part-time job for mental health recovery.
There’s a schedule. There are expectations. People show up consistently, do the work, and build skills over time. But they still live at home.
What makes an IOP an IOP
The baseline definition matters because many programs use similar language. SAMHSA defines mental health IOPs as structured treatment delivering a specified number of hours of therapy weekly, and evidence reviewed in the literature shows IOPs can be as effective as inpatient care for some people. One cited Psychiatric Services finding reports 60 to 70 percent success rates for conditions such as depression and anxiety when care is professional and customized (PMC review on IOPs).
That doesn’t mean every person will have the same experience. It does mean IOP is a serious clinical level of care, not a lighter version of treatment.
What a typical week looks like
Most mental health IOPs run across several days each week. Many programs schedule care in half-day blocks so people can still manage parts of normal life.
A typical routine often includes:
- Group therapy on multiple days where clients practice coping skills, communication, emotional regulation, and relapse prevention
- Individual sessions to work on personal goals, symptom patterns, and treatment planning
- Psychoeducation that helps people understand diagnoses, triggers, medications, stress responses, and recovery habits
- Case management or care coordination for practical needs like scheduling, referrals, or discharge planning
Some programs also include family work, medication support, and well-being services.
The key difference from residential care
The biggest distinction is living arrangement. In residential treatment, the person stays at the facility. In an IOP, the person returns home each evening.
That changes the rhythm of treatment in an important way. Recovery skills aren’t kept inside a treatment bubble. They’re tested against traffic, family stress, work emails, loneliness, routines, and all the ordinary pressures that can trigger symptoms.
An IOP gives people a place to practice recovery while still living in the environment where recovery has to work.
Why the schedule matters clinically
People sometimes hear “more sessions” and think the benefit is just extra talking. It’s more than that.
Frequent treatment creates repetition. Repetition helps people notice patterns faster. They catch distorted thinking sooner, identify warning signs earlier, and stop assuming a bad day means failure.
That’s one reason iop programs for mental health can create momentum. The person doesn’t wait a full week between therapeutic contact. They get support, apply it, and come back while the experience is still fresh.
Is an Intensive Outpatient Program Right for You
Not everyone needs an IOP. Some people do well with weekly therapy. Others need a higher level of care first. The right fit depends less on the diagnosis label and more on what daily life looks like right now.
A useful way to think about it is this: an IOP often fits when symptoms are too disruptive to ignore, but the person can still participate safely in outpatient treatment and follow a structured plan.
Four common profiles
The person stepping down from hospital or detox
This person may be medically stable and no longer need full-day or overnight care. But going from constant support to almost none can feel abrupt. An IOP provides a bridge.
The person whose world is shrinking
Work is getting harder. Social plans keep getting canceled. Sleep is off. Mood swings, panic, or intrusive thoughts are taking over the week. Weekly therapy may feel supportive, but not sufficient.
The person with dual diagnosis
Mental health symptoms and substance use often interact. Anxiety may fuel drinking. Depression may deepen after drug use. Trauma may sit underneath both. These situations usually need integrated treatment rather than separate tracks.
The person trying to stay functional while getting help
Some adults need strong support but still want to keep a connection to work, classes, children, or home responsibilities. They need structure without full removal from daily life.
Signs that point toward IOP
A person may want to ask whether these statements sound familiar:
- “Coping skills make sense in theory, but they disappear under stress.”
- “There’s been a recent crisis, and things still feel shaky.”
- “Home is safe enough, but not easy.”
- “Symptoms keep interfering with daily responsibilities.”
- “There’s a pattern of relapse, shutdown, or escalating conflict.”
If several fit, an IOP evaluation is worth considering.
When an IOP may not be the first step
IOP isn’t the right entry point for everyone. Some people first need a higher level of support because symptoms are too severe, safety is uncertain, or detox or stabilization is still needed.
That’s why a strong assessment matters. Good programs don’t squeeze everyone into the same schedule. They look at current risk, functioning, substance use, psychiatric symptoms, and support at home before recommending a level of care.
The best match isn’t the most intensive option available. It’s the level of care that gives enough support without creating unnecessary disruption.
A practical way families can think about fit
Families often ask one big question in different forms: “Can this person be at home and still recover safely?” That’s often the heart of the decision.
If the answer is “yes, but they need more structure than once-a-week therapy,” an IOP may be a strong fit. If the answer is “not yet,” then another level of care may come first.
Inside the Therapy Room What to Expect
People often know they need help but still wonder what happens once treatment starts. That uncertainty can keep them stuck. The therapy room is usually much less mysterious than people fear.
Most IOPs combine several forms of care because mental health problems rarely improve through one conversation a week alone. Symptoms affect thoughts, habits, relationships, sleep, body regulation, and decision-making. Treatment needs enough range to meet that reality.

Group therapy is the engine
Group therapy is often the core of an IOP. That can worry people at first, especially those who are private, anxious, or used to hiding pain behind competence.
But group isn’t just “talking in front of strangers.” It gives people a chance to hear their own struggles reflected back in ordinary language. Shame tends to lose some of its grip when someone realizes others have had similar thoughts, reactions, or fears.
In group, clients often work on:
- Recognizing triggers that set off panic, anger, avoidance, cravings, or shutdown
- Practicing communication so conflict doesn’t immediately become collapse or escalation
- Building emotional regulation through structured coping skills
- Testing beliefs such as “nothing helps,” “I always ruin things,” or “no one would understand”
For some age groups, the peer element matters even more. Data-driven program optimization has shown that increasing peer group therapy for patients ages 18 to 25 can improve recovery metrics by reducing isolation (Decade2Connect on optimizing IOPs).
Individual therapy personalizes the work
Group gives breadth. Individual therapy gives depth.
A clinician helps the person map out their specific patterns. One client may need trauma work and boundary-setting. Another may need help with obsessive thinking, avoidance, or major depression that’s flattened motivation. Another may need dual-diagnosis treatment that accounts for both mental health symptoms and substance use.
The point isn’t to repeat group in private. It’s to customize the program to the person.
Family therapy changes the environment around recovery
Mental health symptoms don’t happen in a vacuum. They land in homes, partnerships, and parent-child relationships. Family sessions can reduce misunderstanding and improve support.
Evidence-based IOP models matter here. The Matrix Model integrates CBT and family education, and family therapy components have been associated with boosting long-term success rates by as much as 35 percent through better communication and attachment repair (NCBI Bookshelf on treatment approaches).
That doesn’t mean every family session is easy. It means the home environment can become more supportive when people learn how to respond differently.
CBT and DBT in plain language
Two of the most common treatment models in iop programs for mental health are CBT and DBT.
CBT helps people notice the connection between thoughts, feelings, and behavior. If someone automatically thinks, “This meeting will go badly, so there’s no point trying,” CBT helps challenge that chain before it drives avoidance. A helpful overview of this approach appears in this guide to cognitive behavioral therapy.
DBT is often useful when emotions hit fast and hard. It teaches concrete skills for distress tolerance, mindfulness, and relationship effectiveness. Instead of telling someone to “calm down,” it gives them methods for getting through intense moments without making things worse.
Good therapy doesn’t ask a person to stop having symptoms by force. It teaches what to do when symptoms show up.
Medication support and dual-diagnosis care
Some clients also need medication management or MAT as part of treatment. This matters when anxiety, depression, trauma, bipolar symptoms, or substance dependence need coordinated care rather than fragmented treatment.
The strongest outpatient programs don’t treat mental health and substance use as separate stories when they clearly overlap. They build one plan.
Extensive supports help skills stick
Talk therapy matters. So does the nervous system. People who are flooded, numb, exhausted, or physically dysregulated often need more than insight.
That’s why some programs add supports such as:
- Yoga or movement-based work to reconnect body awareness with emotional regulation
- Nutrition guidance when eating patterns and mood are affecting each other
- Outdoor or experiential therapy to help clients practice presence, routine, and stress reduction in daily settings
These additions don’t replace clinical treatment. They make it more usable.
Finding the Right Level of Support
Mental health care works best when the level of support matches the level of need. That sounds simple, but it’s one of the places families get stuck. Too little structure can leave someone floundering. Too much can feel overwhelming or unnecessary.
A practical comparison helps.
Comparing common levels of care
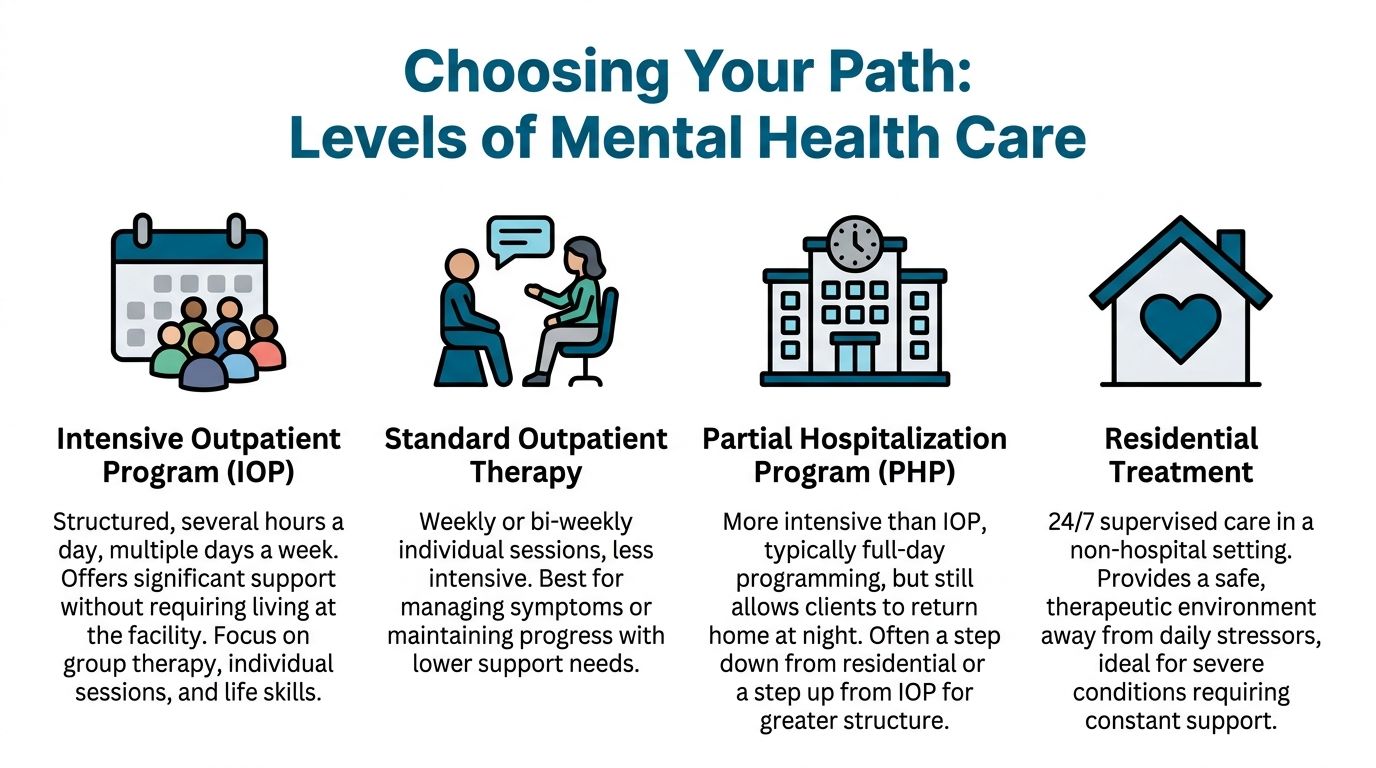
| Level of Care | Time Commitment | Living Situation | Best For |
|---|---|---|---|
| Intensive Outpatient Program (IOP) | Several hours a day, multiple days a week | Lives at home | People who need structured support without overnight care |
| Standard Outpatient Therapy | Usually weekly or bi-weekly sessions | Lives at home | People with lower support needs or those maintaining progress |
| Partial Hospitalization Program (PHP) | More intensive day programming | Lives at home | People who need more daily structure than IOP provides |
| Residential Treatment | Full-time care | Lives at the facility | People needing constant support and a highly contained setting |
Where IOP sits in the continuum
IOP often works as the middle lane. It’s more intensive than standard outpatient care, but less restrictive than PHP or residential treatment.
That role matters clinically. A landmark study reported that people who completed an IOP achieved a 55% abstinence rate at 6 months post-treatment, supporting IOP as an effective step in the continuum with outcomes comparable to higher levels of care in appropriate cases (Journal of Substance Abuse Treatment summary).
This doesn’t mean IOP replaces every higher level of care. It means it belongs in the same serious treatment conversation.
How to decide between outpatient, IOP, PHP, and residential
A few questions usually clarify the choice.
- How safe is the home environment? If home is stable enough, outpatient models become more realistic.
- How quickly are symptoms escalating? Faster escalation often points toward more structure.
- Can the person function between sessions? If long gaps lead to unraveling, a higher frequency of care may help.
- Is there dual diagnosis involved? Combined mental health and substance use needs often require more coordinated support.
For readers comparing day-program options, this overview of a partial hospitalization program php can help distinguish when a person may need more intensity than IOP offers.
Practical examples
A person who’s missing work, isolating, and struggling to apply coping skills may do well in IOP.
A person who can’t maintain safety, needs near-constant monitoring, or is still acutely unstable may need residential or another higher level first.
A person who is improving and mainly needs maintenance may be fine in standard outpatient therapy.
The level of care should answer one question above all: what amount of structure gives this person the best chance to stabilize and keep moving?
Mental health systems can also look different depending on where someone lives. For people navigating care across borders or while living abroad, resources on mental health services for expats can offer useful context about access barriers, continuity of care, and what to ask when systems feel unfamiliar.
{kind=link}
Questions to Ask Before Enrolling in an IOP
Choosing an IOP shouldn’t feel like guessing. A good admissions conversation should answer practical and clinical questions clearly. If a program avoids specifics, that’s useful information too.
This is especially important during the transition from inpatient care or detox. Many resources mention the “step-down” concept, but don’t explain readiness criteria or how relapse prevention is handled during that vulnerable period. That gap is one reason individualized planning matters so much (discussion of the transition challenge).
Questions that reveal program quality
A strong checklist helps families cut through marketing language.
- How is placement determined? The program should explain how it decides whether IOP is appropriate or whether another level of care would be safer.
- What diagnoses and co-occurring concerns does the team treat regularly? Mental health treatment should account for trauma, mood disorders, anxiety, substance use, and overlapping patterns where relevant.
- Which therapies are used, and how are they matched to the client? Vague answers aren’t enough. The program should be able to name approaches and explain why they fit.
- How is family involved? Families don’t need to run treatment, but they often need guidance, education, and healthier communication patterns.
- What happens if symptoms worsen? A responsible program has a plan for escalation, referral, and continuity.
- What does discharge planning look like? Good care doesn’t stop at the last session.
Questions about trauma, transitions, and coordination
A lot of people entering treatment have trauma histories, even if trauma isn’t the first thing they mention. That’s why families should ask how the program handles shame, triggers, emotional overwhelm, and treatment pacing. This overview of the benefits of trauma-informed care gives a useful framework for what thoughtful treatment should look like.
Other questions worth asking include:
- How does the team handle medication coordination?
- How are relapse risks or warning signs tracked over time?
- What support exists for work, school, or family reintegration?
- How does the program communicate with outside providers when appropriate?
What a strong answer sounds like
The best responses are concrete. They describe the assessment process, schedule, therapeutic models, family options, and how the team adjusts treatment when someone isn’t progressing as expected.
A program discussion should also cover practical logistics:
- Insurance verification
- Program schedule
- Expected attendance
- Confidentiality
- Aftercare planning
One Orange County option that provides outpatient mental health and dual-diagnosis services is Zoe Behavioral Health. Its services include IOP, PHP, outpatient counseling, MAT support, and integrated elements such as yoga, nutrition guidance, and outdoor therapy, which can be relevant for adults seeking structured care close to home.
A useful admissions call leaves a person feeling clearer, not pressured.
Starting Your Recovery Journey Today
Once a person decides to explore iop programs for mental health, the next step should be simple. Complicated intake processes can stop people at the exact moment they’re finally ready.
A smoother path usually starts with a confidential call. The purpose isn’t to force a decision. It’s to understand what’s happening, what level of support may fit, and what practical barriers need to be handled first.

A simple admissions path
Most admissions processes move through a few core steps.
First comes the initial conversation. The team gathers basic information about symptoms, recent treatment, substance use if relevant, and immediate concerns.
Next comes insurance verification. This helps the person understand benefits and possible coverage before treatment begins.
Then comes the clinical assessment. That’s where the appropriate fit decision happens. The team looks at symptom severity, safety, current functioning, history, and what kind of structure is likely to help.
After that, scheduling begins. If IOP is appropriate, the person gets a start date and a clear picture of what the week will look like.
Why individualized treatment planning matters
The strongest IOPs don’t run every client through the same formula. They adjust care based on response, participation, symptoms, and age-specific needs when relevant.
That kind of refinement matters in practice. Data-informed optimization in IOPs has shown that increasing peer group therapy for patients ages 18 to 25 can improve recovery metrics by reducing isolation (data-driven IOP optimization).
That principle applies more broadly too. When treatment teams track progress carefully, they can modify the plan instead of waiting for a setback to make the need obvious.
What helps people take the first step
People are more likely to follow through when the process feels manageable.
- Clarity helps. They know what happens on the first call.
- Speed helps. They don’t have to wait in uncertainty.
- Respect helps. They feel heard, not sold to.
- Fit helps. The recommendation matches the problem.
A person doesn’t need to have the whole recovery plan figured out before reaching out. They only need enough readiness to start the conversation.
A confidential conversation with Zoe Behavioral Health can help Orange County adults and families understand whether IOP, PHP, outpatient counseling, or another step in care makes sense right now. The admissions team can review symptoms, discuss scheduling, verify insurance, and help identify a practical next step without adding more confusion to an already difficult moment.