
A family in California often reaches the same breaking point after months or years of confusion. A son completes addiction treatment, comes home sober, and then spirals when panic, depression, or trauma symptoms return. A spouse finally starts therapy for mental health, makes progress, and then alcohol or pills pull everything off course again. Everyone involved starts asking the same question: why does treatment keep helping for a while, but not hold?
In many cases, the missing piece is not effort. It is integration. When a person has both a substance use disorder and a mental health disorder, separate treatment tracks rarely produce stable recovery. California families looking into california dual diagnosis treatment centers are usually not starting from zero. They are trying to stop a cycle that already proved standard approaches were not enough.
The Overlapping Crises of Mental Health and Addiction
A dual diagnosis crisis rarely looks dramatic at first. It often looks inconsistent.
Someone drinks to sleep because anxiety is relentless. Then alcohol worsens mood instability. Someone uses opioids to numb trauma symptoms, then experiences deeper depression, isolation, and hopelessness between doses. A parent watching this from the outside may assume the primary problem is addiction. Another may believe the mental health condition is the true issue. When both are active, treating only one leaves the other free to restart the cycle.

Why families miss the pattern
Dual diagnosis is easy to miss because the symptoms overlap. Poor sleep, irritability, emotional numbness, impulsive behavior, social withdrawal, and concentration problems can come from substance use, psychiatric distress, or both.
That is why many families spend months pursuing the wrong sequence. They try sobriety first without psychiatric care. Or they focus on therapy while ongoing substance use keeps destabilizing progress. A more useful starting point is understanding the connection between mental health and addiction.
The scale of the problem in California
The need for california dual diagnosis treatment centers is not niche. In California, about 8.5% of all residents experience co-occurring mental health and substance use disorders, slightly above the national average of 7.7%. The same source notes that over 5.36 million Californians aged 12+ had a substance use disorder in 2021, but only 10% received specialty care, leaving over 4.8 million untreated (American Addiction Centers on California dual diagnosis rehab).
Those figures matter for one practical reason. Families are not overreacting when they feel the system is hard to find their way through. The demand is real, and many people with co-occurring disorders never reach treatment that addresses both conditions at once.
Key takeaway: Repeated relapse after prior treatment does not automatically mean the person is resistant to help. It often means the treatment model did not address both disorders together.
What Is a Dual Diagnosis
Dual diagnosis means a person is living with both a substance use disorder and a mental health disorder at the same time. Clinicians also call this a co-occurring disorder.
The simplest way to understand it is to picture two roots wrapped around each other underground. One root is the addiction. The other is the psychiatric condition. Pulling on only one root leaves the other in place, and the problem grows back.
Why separate treatment falls short
A person may drink because social anxiety feels unbearable. Another may misuse stimulants to push through depression and fatigue. Someone with trauma symptoms may rely on opioids, cannabis, or alcohol to shut off nightmares, hypervigilance, or emotional pain.
If treatment addresses only the substance use, the original distress remains. If treatment addresses only the mental health symptoms while active use continues, therapy often becomes unstable, inconsistent, or unsafe. Integrated care matters because both problems reinforce each other.
A practical analogy helps. Trying to treat dual diagnosis in separate silos is like fixing a car’s alignment while ignoring worn tires. One repair may help briefly, but the underlying instability keeps showing up on the road.
How the disorders interact
The interaction usually follows a few common patterns:
- Self-medication: A person uses substances to reduce anxiety, trauma symptoms, sadness, racing thoughts, or insomnia.
- Substance-induced worsening: Alcohol, stimulants, opioids, or other drugs intensify depression, panic, irritability, paranoia, or emotional swings.
- Relapse loop: The mental health symptoms trigger use, and the use deepens the psychiatric symptoms.
- Fragmented care: Different providers treat different issues without one coordinated plan.
The family often sees this as unpredictability. Clinically, it is more accurate to see it as an untreated system.
Common pairings seen in practice
Some combinations appear repeatedly in california dual diagnosis treatment centers:
Anxiety and alcohol use
Alcohol may look like fast relief. Over time it often worsens sleep, rebound anxiety, and dependence.
Depression and stimulant use
Stimulants can temporarily create energy or confidence, but crashes often deepen despair and emotional exhaustion.
PTSD and opioid use
Opioids may numb trauma-related pain, but they can also narrow coping skills and make daily functioning more fragile.
Mood instability and polysubstance use
People sometimes switch substances depending on the symptom of the day. They may use one drug to get up, another to come down, and alcohol to sleep.
What integrated care means
A dual diagnosis program does more than offer addiction counseling plus a separate therapy appointment. It coordinates care around one clinical picture.
That usually includes:
- A full assessment of mental health history, substance use patterns, medications, risk factors, and current functioning.
- A treatment plan that addresses both disorders at the same time.
- Psychiatric support when medication evaluation or medication management is needed.
- Therapy that links triggers and symptoms, rather than treating them as unrelated problems.
- Case management and continuity, especially during transitions between levels of care.
Clinical reality: A person does not need to know which disorder came first in order to start effective treatment. What matters is whether the program can assess and treat both together.
Common Signs of a Co-Occurring Disorder
Families often sense that something more complex is happening before they know the term dual diagnosis. They notice that sobriety does not fully stabilize mood. Or they see mental health treatment stall because the person keeps returning to alcohol, pills, or drugs under stress.
That observation is important. It should not be used for self-diagnosis, but it should prompt a thorough professional assessment.

Behavioral signs families often notice
Some signs are easiest to spot through patterns over time:
- Using substances to cope with emotions: The person drinks, uses, or misuses medication during anxiety, grief, anger, shame, or social stress.
- Rapid reversals after treatment: They complete a program or a sober stretch, then relapse when emotional symptoms return.
- Unpredictable functioning: Good days are followed by major crashes in motivation, sleep, work attendance, or relationships.
- Multiple coping systems failing at once: Therapy, medication routines, and sobriety efforts all break down together during distress.
Emotional and psychiatric clues
Other signs show up more clearly in the person’s inner life:
- Persistent sadness, hopelessness, or emotional numbness
- Panic, dread, restlessness, or intense social fear
- Trauma responses such as nightmares, hypervigilance, or shutdown
- Irritability that seems larger than the situation
- Severe shame after substance use, followed by more use
- Difficulty regulating mood even during short periods of abstinence
A key detail is timing. If symptoms remain intense during sobriety, or if they worsen sharply when substances are removed, a co-occurring disorder should be considered.
Impact on work, family, and daily life
Dual diagnosis rarely stays contained to one area. It spreads into the person’s routines.
Warning signs can include:
- Work disruption: missed shifts, poor concentration, conflict, or sudden performance decline
- Family strain: secrecy, isolation, defensiveness, or frequent emotional crises
- Treatment inconsistency: stopping therapy, skipping appointments, refusing medications, or cycling through programs without traction
- Loss of structure: disrupted meals, unstable sleep, financial chaos, or legal stress tied to substance use
Practical tip: When calling a treatment center, families should describe patterns instead of labels. “He drinks every time panic builds and becomes more depressed afterward” is more useful than “He probably has dual diagnosis.”
What a proper assessment should look for
A quality assessment does not rush to a label. It looks at the full picture.
That includes substance history, mental health symptoms, trauma exposure, medication use, prior treatment, current safety concerns, and the person’s living environment. The goal is not to prove the family right. The goal is to identify what level of care can safely interrupt the cycle.
The Dual Diagnosis Treatment Continuum in California
Finding the right level of care matters as much as finding the right diagnosis. A person who needs daily structure may fail in a low-intensity setting. A person who is stable enough for outpatient care may resist treatment entirely if only residential options are presented.
California’s treatment system works best when families understand it as a continuum instead of a single decision.
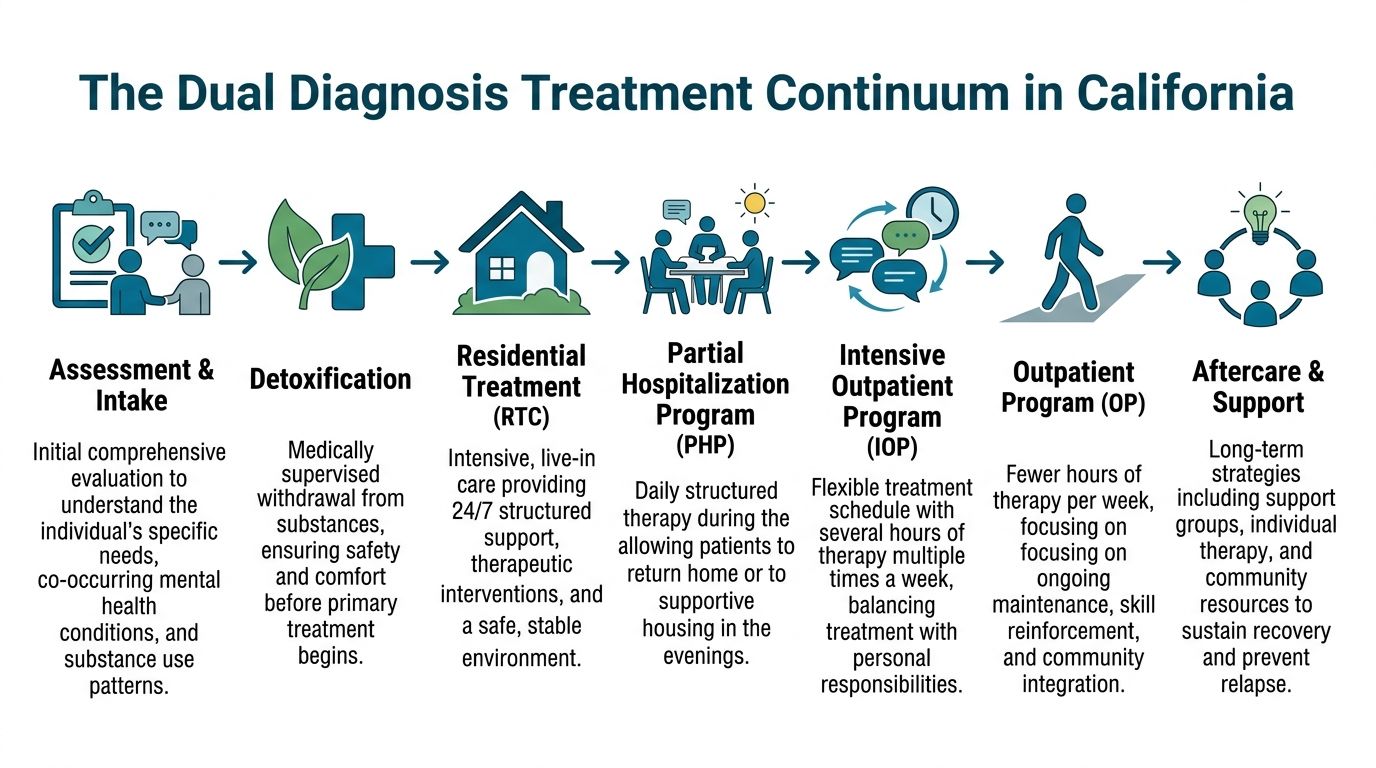
Assessment and detox referrals
The first task is matching the person to a safe starting point.
If withdrawal risk is high, outpatient treatment usually begins with a detox referral. That is common with alcohol, benzodiazepines, opioids, or heavy multi-substance use. Detox addresses immediate medical stabilization. It does not replace therapy for the underlying co-occurring disorder.
After detox, the strongest outcomes usually come from moving directly into structured treatment instead of waiting for motivation to carry the person alone.
PHP, IOP, and outpatient care
For many adults in Orange County and across California, outpatient care is the most practical path because it allows treatment without completely stepping out of life.
A strong outpatient continuum often includes:
Partial Hospitalization Program
PHP offers the highest level of structured outpatient care. It fits people who need frequent clinical contact, close monitoring, and a full therapeutic schedule during the day, while still returning home or to sober living at night. More detail on this level of care appears in this overview of a partial hospitalization program PHP.
Intensive Outpatient Program
IOP is a step down from PHP. It gives clients multiple therapy sessions each week with more flexibility for work, school, family care, and gradual re-entry into normal routines.
Standard outpatient counseling
This level works best for maintenance, ongoing therapy, medication follow-up, relapse prevention, and longer-term support after higher-intensity treatment.
Comparing Levels of Outpatient Care
| Feature | Partial Hospitalization Program (PHP) | Intensive Outpatient Program (IOP) |
|---|---|---|
| Structure | High structure during the day | Moderate structure across the week |
| Best fit | People needing intensive support without overnight stay | People stable enough to balance treatment with daily responsibilities |
| Clinical focus | Stabilization, symptom management, relapse prevention, psychiatric coordination | Continued therapy, skill building, accountability, community reintegration |
| Daily life | Treatment becomes the main daytime commitment | Treatment works around employment, parenting, or school when appropriate |
| Step in continuum | Often follows detox or residential care | Often follows PHP or serves as the entry point for stable clients |
Where MAT fits in dual diagnosis care
For people with opioid use disorder and co-occurring mental health symptoms, Medication-Assisted Treatment can be a major stabilizing tool. According to the California Bridge Program overview, MAT using buprenorphine or naltrexone can reduce withdrawal severity by up to 80% and cravings by 50% to 70%. The same source notes that, when integrated into PHP or IOP, MAT is associated with 60% to 75% retention at 6 months, compared with 20% to 30% for detox-only approaches.
Those numbers matter because retention is not a technical metric for families. It often means the difference between someone staying engaged long enough to get psychiatric symptoms under control, repair sleep, build coping skills, and create a recovery routine that can hold under stress.
What works and what does not
The most effective continuum has continuity. The same treatment team, or at least a closely coordinated one, should know the person’s trauma history, substance triggers, medication plan, relapse warning signs, and family dynamics.
What tends not to work:
- Detox without a clear next step
- Outpatient therapy without addiction expertise
- Addiction counseling without psychiatric support
- A level of care chosen for convenience rather than clinical need
What usually works better:
- Starting with a thorough assessment
- Moving through levels of care as stability improves
- Using MAT when clinically appropriate
- Including individual therapy, group work, psychiatric care, and practical case management in one plan
One outpatient example in Orange County is Zoe Behavioral Health, which provides dual diagnosis treatment through detox referrals, PHP, IOP, outpatient counseling, and sober living coordination within a DHCS-licensed setting.
Key takeaway: The right question is not “inpatient or outpatient?” The right question is “what level of structure is needed right now, and how will care step down safely over time?”
How to Find Quality Dual Diagnosis Treatment in California
A polished website is not enough. A calm phone call is not enough. Families looking at california dual diagnosis treatment centers need a way to separate programs that effectively treat co-occurring disorders from programs that merely mention the term.
California has broad treatment availability on paper, but not every option offers the same depth of care. According to this California dual diagnosis treatment overview, the state has over 2,200 listed dual diagnosis centers, yet there is a 28% rise in outpatient waitlists, and Orange County facilities are at 85% capacity. That shortage especially affects working adults who need PHP or IOP rather than a residential-only model.

Non-negotiable quality markers
Families should look for a few concrete standards before anything else.
DHCS licensing
A California program should be properly licensed for the services it provides. That does not guarantee excellence, but it is a baseline safeguard.
A multidisciplinary team
Dual diagnosis care works best when therapists, case managers, and psychiatric providers coordinate around one plan instead of treating isolated symptoms.
Evidence-based therapy
Programs should be able to clearly describe how they use therapies such as CBT, DBT, trauma-informed counseling, relapse prevention work, and medication support when needed.
Psychiatric involvement
If the person has panic, depression, trauma symptoms, mood instability, or medication history, psychiatric assessment cannot be an afterthought.
Clear step-down planning
A quality center should explain what happens after the first phase of care. Families should hear a plan for transitions, not vague promises.
Signs a program may not be fully dual diagnosis capable
Some red flags appear quickly during the admissions process:
- The program talks almost entirely about sobriety but not mental health treatment.
- Staff cannot explain how therapy and psychiatric care are integrated.
- The assessment feels rushed and focused only on substance use frequency.
- Medication questions are brushed aside.
- The program has no clear answer about what level of care comes next.
Why outpatient access matters in Orange County
Many adults cannot disappear from life for an extended residential stay, even when they need serious help. They may be managing work, custody, elder care, school, or financial pressure. Others are clinically appropriate for outpatient treatment after detox or residential care, but lose momentum because the next step is hard to secure.
This is the gap families should pay attention to. A program can be clinically solid and still be the wrong fit if it requires a life arrangement the client cannot sustain.
Strong outpatient dual diagnosis care should allow room for real-world integration:
- sleeping at home or in supportive housing
- rebuilding routines gradually
- attending structured treatment during the day
- coordinating family communication
- managing medications with supervision
- planning for work re-entry without rushing it
Practical filter: Ask whether the center’s daily schedule fits the person’s actual life. A good clinical model still fails if the logistics make attendance unrealistic.
What Insurance Verification Means and Admissions for Treatment
Insurance worries stop many families before treatment even begins. They assume the process will be confusing, expensive, or impossible to understand over the phone.
It does not have to start that way. The first step is usually much simpler than expected.
What insurance verification means
Insurance verification is the process of checking a person’s behavioral health benefits before admission. The admissions team gathers policy information, confirms whether the plan is active, and determines what levels of care may be covered.
For families with PPO plans, this step often answers the most urgent questions:
- Is outpatient dual diagnosis treatment covered?
- Is PHP or IOP included?
- Are there deductibles, copays, or authorization requirements?
- Is medication management part of the behavioral health benefit?
A useful overview of this process appears in this resource on insurance coverage.
What to expect during admissions
A strong admissions process should feel organized, not pressuring.
The call usually covers:
- Current substance use and safety concerns
- Mental health symptoms and treatment history
- Withdrawal risk and whether detox is needed first
- Insurance information
- Recommended level of care and next steps
Families should expect direct questions. That is a good sign. Accurate placement depends on honest clinical screening.
What helps the process move faster
It helps to have a few details ready:
- insurance card
- current medications
- recent treatment history
- substances being used and approximate frequency
- any urgent psychiatric concerns
- contact information for family support, if the client wants that involved
If the family does not know every answer, that should not stop the call. Admissions teams work with incomplete information all the time. The priority is getting the clinical picture clear enough to recommend a safe next step.
Reassurance for families: The purpose of admissions is not to trap anyone into treatment. It is to reduce uncertainty, identify the right level of care, and remove delays that keep the person stuck.
Your Next Steps and Questions to Ask Providers
Choosing among california dual diagnosis treatment centers becomes easier when families stop asking broad questions like “Do you treat mental health too?” and start asking operational ones.
The quality of care usually reveals itself in the specifics.
Questions worth asking on the first call
- How do you assess both mental health symptoms and substance use at intake?
- Do you provide integrated treatment for both conditions at the same time?
- Is psychiatric evaluation or medication management available if needed?
- How do you decide between PHP, IOP, and standard outpatient care?
- What happens if the client needs detox before starting outpatient treatment?
- How do you handle relapse risk during treatment?
- What therapies do you use for trauma, anxiety, depression, or mood instability?
- How do family communication and case management work?
- What does the step-down plan look like after the initial level of care?
- How quickly can admissions and insurance verification begin?
The answers that usually indicate stronger care
Good programs answer directly. They can explain how therapy, psychiatric oversight, and addiction treatment connect in the same plan. They can also describe transitions between levels of care without sounding vague or improvised.
That matters because untreated mental health symptoms drive 70% to 85% of substance relapses, and high-quality integrated care that blends therapies such as CBT and EMDR with MAT can boost remission rates to 55% at 12 months, more than double sequential treatment approaches (overview of integrated concurrent therapy).
What families should remember
A failed treatment episode does not mean recovery is out of reach. It often means the care was incomplete, the level of support was mismatched, or the mental health side of the illness stayed untreated.
The next right step is not to wait for a worse crisis. It is to ask sharper questions, verify benefits, and get a full assessment from a program that understands both sides of the condition.
If a loved one is cycling through relapse, emotional instability, or repeated treatment attempts that never seem to hold, the next step is a confidential conversation with Zoe Behavioral Health. Their admissions team can help review symptoms, discuss outpatient dual diagnosis options in Orange County, and verify insurance so families can move from fear and uncertainty toward a clear treatment plan.