Recovery often reaches a confusing point. Weekly therapy may no longer feel like enough, but leaving home for full-time residential treatment may seem impossible because of work, family, school, or simple uncertainty about whether that level of care is necessary.
That gap is where many adults start asking what is partial hospitalization program care, and whether it could fit real life in Orange County. A Partial Hospitalization Program, usually called PHP, is designed for people who need strong daily support without overnight stays. It gives structure, therapy, psychiatric oversight, and accountability during the day, then allows clients to return home in the evening.
For someone who has just finished detox, someone whose depression or anxiety is getting harder to manage, or someone slipping back toward substance use despite outpatient counseling, PHP can be the bridge that keeps a crisis from becoming something worse. Families often need a clear roadmap at this stage. A practical guide to finding help for substance abuse admissions can make that first step feel more manageable.
Finding the Right Level of Addiction and Mental Health Care
Choosing treatment isn't only about how severe symptoms look from the outside. It’s also about how much support a person needs to stay safe, function day to day, and put into practice the coping skills they’re learning.
Some adults need medical detox because withdrawal is the first urgent issue. Others need residential treatment because home isn’t stable yet. Then there are people in the middle. They’re struggling enough that standard outpatient care isn’t containing the problem, but they don’t need round-the-clock supervision. PHP serves that middle ground.
When the middle ground matters
A common situation looks like this: a person attends therapy once a week, maybe sees a psychiatrist once a month, and still feels overwhelmed between appointments. Cravings return at night. Panic builds in the morning. Mood swings affect work, parenting, or relationships. Progress happens in sessions, then falls apart at home.
PHP is built for that exact pattern. It adds daily clinical structure without removing the person from ordinary life completely.
Practical rule: If someone needs more support than weekly therapy but can still sleep safely at home, PHP may be worth assessing.
Why this level of care can feel more realistic
Many people delay treatment because they assume the only serious option is inpatient rehab. That assumption keeps them stuck. PHP offers a different path. It creates a strong treatment routine while still letting someone stay connected to family responsibilities, practice recovery skills in their daily environment, and begin rebuilding normal life instead of putting it on hold.
For Orange County residents, that balance often matters. Commutes, jobs, caregiving, and housing realities can make all-or-nothing treatment decisions feel impossible. PHP gives clinicians a way to match care more precisely to what the person needs right now.
Understanding the Partial Hospitalization Program Structure
PHP provides a substantial daily treatment schedule built to stabilize symptoms, strengthen recovery skills, and give people consistent clinical support while they continue living at home.
For many Orange County residents, that structure answers the question they are really asking: What will my week look like? In a PHP, you spend much of the day in treatment, then return home in the evening. That matters because recovery is not only about what happens in session. It is also about how you handle the drive home, dinner with family, a stressful text message, poor sleep, or cravings that show up after dark.
What happens during the day
A PHP follows a planned clinical schedule, not a loose collection of appointments. The goal is to give enough repetition and support that new skills start to hold under real-life pressure.
A typical treatment plan may include:
- Diagnostic assessment and treatment planning so the team can clarify substance use patterns, mental health symptoms, safety needs, and immediate goals
- Group therapy focused on coping skills, emotional regulation, communication, relapse prevention, and accountability
- Individual counseling to work through personal triggers, trauma, family stress, motivation, or setbacks from the previous evening
- Medication management if psychiatric medication or medication-assisted treatment is part of care
- Family sessions when home relationships affect recovery or the person needs more support outside treatment hours
- Skills practice using approaches such as cognitive behavioral therapy
As described in this discussion of how partial hospitalization programs work, PHPs commonly use a multidisciplinary, evidence-based model that combines evaluation, individualized care planning, therapy, and medication support.
Why the structure helps
The schedule is intensive for a reason. A person may learn a grounding skill in the morning, feel tested by anxiety or conflict that evening, and return the next day ready to review exactly what happened. That quick feedback loop helps treatment move from theory into daily practice.
It works a bit like supervised rehearsal. You practice new responses with clinical support, try them in ordinary life, then come back and adjust.
That is one reason PHP can feel like a practical bridge for people who are not safe with only weekly therapy, but do not need overnight monitoring. They get a high level of contact with clinicians while still building recovery in the environment where they live.
If you are in Orange County and unsure whether this structure fits your situation, a clinical assessment can clear up the confusion quickly. Zoe Behavioral Health helps residents determine whether PHP matches their current needs and connect with an appropriate local program.
PHP Compared to Other Addiction Treatment Programs
Most confusion about PHP comes from not knowing where it fits in the larger continuum of care. People hear terms like detox, residential, IOP, and outpatient, then try to guess which one applies. A cleaner approach is to compare what each level is designed to do.
Treatment Levels of Care Comparison
| Level of Care | Time Commitment | Living Situation | Primary Focus |
|---|---|---|---|
| Medical Detox | Short-term, highly supervised treatment | Usually in a medical or monitored setting | Safe withdrawal and medical stabilization |
| Inpatient or Residential Treatment | Full-day, live-in care | Client stays at the facility | Safety, structure, early recovery, and separation from triggers |
| Partial Hospitalization Program | Most of the day, several days each week | Client lives at home or in supportive housing | Intensive stabilization, therapy, psychiatric support, and transition building |
| Intensive Outpatient Program | Fewer hours than PHP, multiple sessions weekly | Client lives at home | Continued recovery work, relapse prevention, and growing independence |
| Standard Outpatient Therapy | Usually one or a few appointments weekly | Client lives at home | Maintenance, check-ins, and ongoing support |
A fuller look at intensive outpatient program rehab can help clarify the step-down level that often follows PHP.
Where PHP sits in the continuum
PHP is often the answer when a person needs serious help but not overnight monitoring. It can act as a step-down from inpatient or detox, or a step-up from outpatient therapy that isn’t working well enough.
That middle placement matters because treatment should match need, not fear. If the level is too low, the person may keep deteriorating. If it’s too high, the person may resist treatment, leave early, or feel disconnected from normal life.
A simple way families can think about it
Families often ask for the shortest summary possible. This framework usually helps:
- Detox handles withdrawal and immediate medical concerns.
- Residential removes a person from daily triggers and provides around-the-clock care.
- PHP delivers strong daytime treatment while preserving home living.
- IOP supports continued progress with less intensity.
- Outpatient helps maintain gains over time.
PHP is less about “how bad things are” and more about “how much structure is needed for progress to hold.”
That distinction reduces a lot of shame. A recommendation for PHP doesn’t automatically mean someone has “failed” outpatient care. It often means symptoms, cravings, or emotional instability now require a tighter clinical framework.
When PHP may be the better fit than IOP
A person may be better suited for PHP than IOP if daily functioning is slipping fast, cravings are strong, psychiatric symptoms are interfering with basic responsibilities, or recent treatment discharge leaves the person vulnerable to relapse. IOP can be excellent care, but some people need a stronger container before they can benefit from a lighter schedule.
By contrast, someone who has already stabilized and can manage longer gaps between sessions may move into IOP more comfortably. The right answer depends on a professional assessment, not guesswork.
A Typical Day in a Partial Hospitalization Program
The phrase “partial hospitalization” can sound intimidating. The day itself usually feels much more human and practical than the name suggests.
A client might arrive in the morning, check in with staff, and join a group focused on current symptoms, stressors, and goals for the day. That opening matters. It helps the treatment team notice who is struggling, who is improving, and who needs extra support before the day moves on.
Morning rhythm and clinical work
The first block of the day often centers on process work or psychoeducation. One group may focus on identifying relapse triggers. Another may teach emotional regulation, cognitive restructuring, communication, or distress tolerance. Clients aren’t expected to perform perfectly. They’re expected to show up authentically and practice.
Later in the morning, a person may meet individually with a therapist, case manager, nurse, or psychiatric provider. That’s where treatment becomes personalized. Medication questions, sleep problems, family conflict, cravings, or recent setbacks can all be addressed directly.
Midday and afternoon treatment
Lunch and breaks are part of the therapeutic rhythm too. They give clients a chance to regulate, connect with peers, and practice ordinary routines without the chaos that often surrounds active addiction or untreated mental health symptoms.
Afternoon sessions may include:
- Relapse prevention groups focused on high-risk situations
- Skills-based work using CBT or DBT concepts
- Family or case management meetings when housing, work, or aftercare planning needs attention
- Well-being activities such as yoga, movement, mindfulness, or nutrition education
A person then returns home in the evening. That’s not a gap in treatment. It’s part of treatment. Home becomes the place where boundaries, coping skills, medication routines, and sober support plans are tested in real life.
Some of the most important PHP work happens after the client leaves for the day. The evening shows what still needs support.
For many adults, that daily repetition reduces fear. The schedule becomes familiar. Staff become known. The treatment environment starts to feel less like a crisis response and more like a steady place to rebuild.
Who Is the Right Candidate for a PHP?
Not everyone who asks about PHP is a fit for it. That isn’t a rejection. It’s a safety issue and a matching issue. The goal is to place the person in the level of care most likely to help.

One verified analysis reported that only 20% to 30% of PHP referrals succeed due to unmet criteria, and it also notes that California placement often involves physician referral and symptom severity requirements, which is why a strong assessment process matters, according to this explanation of partial hospitalization program eligibility.
Signs someone may be a good fit
PHP often works well for adults who:
- Need more than weekly care because symptoms are escalating or relapse risk is rising
- Are stepping down from detox or residential treatment and need a structured bridge back into community life
- Have a stable place to live where evenings can be spent safely
- Are medically stable and don’t need constant nursing or withdrawal management
- Can participate consistently in a daytime schedule and engage in treatment tasks
Situations that may point elsewhere
PHP may not be the right first placement if a person has unsafe withdrawal risk, unstable housing, immediate danger to self or others, or a home environment that actively undermines treatment. In those cases, a higher level of care may be more appropriate before PHP becomes realistic.
Confusion often arises among families. They may hear “outpatient” and assume any home-based treatment will do. But PHP still asks a lot from the client and from the home setting.
A safe bed at night is part of the treatment plan in PHP, not an afterthought.
Why dual diagnosis matters
PHP can be especially useful for co-occurring disorders, also called dual diagnosis. That means the person isn’t only dealing with alcohol or drug use. The person may also be facing depression, anxiety, trauma symptoms, bipolar disorder, or another mental health condition that affects recovery.
When both conditions interact, low-intensity treatment often misses the pattern. A person may stop using for a few days, then panic, crash emotionally, stop taking medication, isolate, and relapse. PHP gives clinicians more frequent contact and more chances to intervene before that cycle grows.
A careful assessment helps determine whether the person needs detox, PHP, IOP, or another path entirely. That’s why the intake process matters as much as the program itself.
Proven Benefits and Outcomes of PHP Treatment
PHP asks for a serious time commitment. Families deserve evidence that the commitment can lead somewhere meaningful.
One strong finding comes from a significant virtual PHP study. It showed a 50% reduction in patient hospitalizations, dropping from 44 hospitalizations in the year before virtual implementation to 22 hospitalizations in the year after. When adjusted for census fluctuations, the hospitalization rate fell from 16.5% of all discharges to 8.9%, as reported in this peer-reviewed study on virtual partial hospitalization.
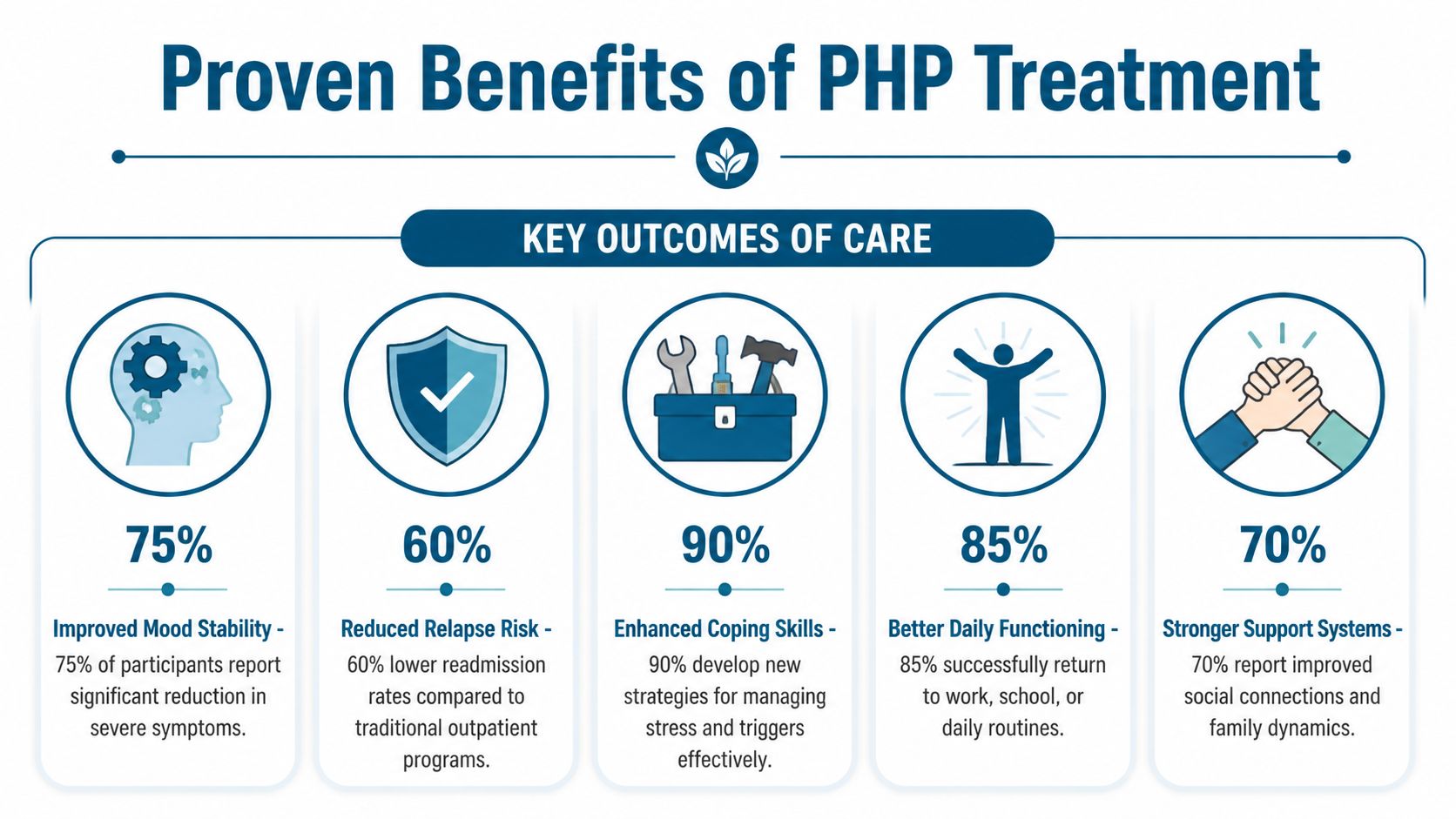
Symptom improvement in real treatment settings
PHP also shows meaningful symptom relief in mood and anxiety care. One study of over 800 adults in a brief PHP found anxiety scores improving from 13.6 at admission to 7.9 at discharge, and depression scores improving from 15.8 to 8.9 in about three weeks, according to this summary of PHP outcomes for depression and anxiety.
That same source also describes a quality report with 29% growth in PHP admissions from 2021, 107 unique consumers across 110 admissions, 84.2% average attendance, and PHQ-9 scores improving from 13.61 to 4.29 at discharge.
Why those outcomes make sense
These results aren’t random. PHP combines several elements that reinforce each other:
- Frequent therapeutic contact catches problems early
- Peer support reduces isolation and shame
- Medication oversight helps stabilize psychiatric symptoms
- Daily repetition helps clients use skills in real situations instead of only discussing them
- Home return each evening reveals what still needs work
A person who learns grounding skills in the morning, uses them after an argument at home, then reviews the result the next day often builds confidence faster than a person who waits a full week between sessions.
PHP doesn’t only provide more treatment hours. It gives clinicians more chances to interrupt relapse patterns while they’re still small.
For adults trying to avoid another hospitalization, another detox admission, or another cycle of short-lived improvement, those outcomes make PHP an option worth taking seriously.
Your Next Step for Treatment in Orange County
A common Orange County scenario looks like this. Someone knows they need more help than a weekly therapy session, but they are not sure whether PHP, IOP, detox, or residential treatment makes sense. A spouse asks if the person can still sleep at home. A parent wants to know how quickly treatment can start. The right next step is an assessment that answers those questions clearly.
PHP sits in the middle of the care spectrum, which is why placement matters. Some adults arrive convinced PHP is the right fit and learn they need detox or a higher level of support first. Others assume they need to be hospitalized and find out they can safely start with PHP or IOP instead. Getting this right saves time, reduces false starts, and gives the person a plan they can follow.
A good assessment works like a map review before a long drive. You may know the destination, but you still need to check the road conditions, the fuel level, and the safest route.
What a strong assessment should clarify
A useful admissions evaluation should answer practical questions, not just collect forms:
- Safety right now, including withdrawal concerns, suicidal thoughts, self-harm risk, or severe psychiatric instability
- Mental health symptoms, such as anxiety, depression, trauma, sleep disruption, panic, and medication history
- Substance use pattern, including what is being used, how often, prior relapses, and what tends to trigger a return to use
- Home and family environment, to see whether evenings at home will support recovery or make it harder
- Daily life logistics, including work, school, transportation, insurance, child care, and outside support
That process helps explain why one level of care fits better than another. It also helps families understand that treatment placement is a clinical decision, not a guess.
For Orange County residents, local details matter more than people often expect. A long commute across the county, an unstable home environment, court requirements, or the need for both addiction and mental health treatment can change what is realistic. PHP often works best as a bridge. It gives a person more structure than standard outpatient care while letting them stay connected to home, family, and real-life responsibilities.
That is often the question people are really asking. Not only "What is a partial hospitalization program?" but "What will my week look like, and can I do this?"
Zoe Behavioral Health in Lake Forest helps answer that question through assessments, outpatient treatment, and care coordination for adults dealing with addiction, mental health conditions, and dual-diagnosis concerns. If PHP is appropriate, the admissions team can explain what to expect. If another level of care makes more sense, they can help with that placement and next steps.
Clarity lowers fear. Once the level of care is matched to the person, treatment usually feels less confusing and much more doable.
A confidential assessment can help determine whether PHP, IOP, outpatient care, or another level of support fits best. For Orange County adults and families looking for clear guidance on addiction and mental health treatment, Zoe Behavioral Health offers admissions support, insurance verification, and individualized care planning.