
Some people know exactly when anxiety and depression started. For others, it arrived gradually. Sleep got lighter. Small tasks started to feel strangely heavy. The mind stayed busy with worry while the body felt drained, flat, and slow. A person wants relief, wants to show up for work, family, or school, but can't seem to move in a straight line.
That combination is exhausting because the symptoms pull in opposite directions. Anxiety pushes the nervous system into overdrive. Depression takes energy, motivation, and hope offline. When both show up together, people often blame themselves for being inconsistent, avoidant, or “not trying hard enough.” That's usually not what's happening. They're stuck in a treatable clinical pattern.
The search for the best therapy for anxiety and depression gets confusing fast. There's weekly counseling, medication, group therapy, trauma work, online programs, and higher levels of care when life starts slipping. The right answer usually isn't one single technique. It's the right combination of therapy, support, structure, and sometimes medical treatment, matched to the severity of what's going on.
The Weight of a Double Diagnosis
A common story sounds like this. Someone wakes up already tense, checks messages, feels dread about the day, and starts mentally rehearsing everything that could go wrong. By afternoon, the same person feels too depleted to answer calls, finish tasks, or meet basic responsibilities. At night, guilt takes over because the day didn't go the way it should have. Then the cycle starts again.
Families often see only pieces of that cycle. They notice irritability, isolation, missed work, drinking that seems to be increasing, or a sudden loss of interest in things that used to matter. What they don't always see is how often anxiety and depression travel together, and how often substance use gets pulled in as an attempted form of self-relief.
For many people, the turning point comes when they stop asking, “Why can't this person just push through?” and start understanding co-occurring disorders as overlapping conditions that need coordinated care.
When anxiety and depression overlap, motivation usually doesn't return through willpower alone. Treatment has to reduce symptoms and rebuild daily functioning at the same time.
What feeling stuck usually means
Being stuck doesn't mean treatment won't work. It usually means the current level of care isn't enough, or the treatment plan is too narrow. A person may be trying to fix severe symptoms with occasional therapy, no psychiatric support, and no structure between sessions. That's a mismatch, not a failure.
What hope looks like in practice
Hope becomes real when treatment gets specific. That means identifying whether the main drivers are worry, panic, hopelessness, avoidance, trauma, sleep disruption, substance use, or all of the above. Once the pattern is clearer, the path gets clearer too.
The strongest treatment plans don't promise a quick fix. They offer a practical route forward. Better symptom control, stronger coping skills, more stability at home, and a level of support that fits the problem.
Your Toolkit for Mental Wellness Evidence-Based Therapies
Psychotherapy works best when it's understood as a set of tools, not a vague conversation. Different therapies target different problems. Some help people challenge distorted thinking. Others help them regulate intense emotions, tolerate distress, or re-engage with daily life when depression has narrowed everything down.
Why CBT usually comes first
Cognitive Behavioral Therapy, or CBT, remains the clearest first-line option when anxiety and depression are driving day-to-day impairment. For generalized anxiety disorder, CBT showed superior long-term effectiveness, and at 3 to 12 months post-intervention it was associated with a greater reduction in anxiety severity than treatment as usual, with a standardized mean difference of −0.60 in the JAMA Psychiatry review and meta-analysis.
CBT helps in two directions at once. On the cognitive side, it identifies thinking errors such as catastrophizing, all-or-nothing thinking, and overestimating danger. On the behavioral side, it reduces avoidance and increases action. That matters because anxiety expands through avoidance, while depression deepens through withdrawal and inactivity.
For people who also need support around addictive patterns and coping habits, structured skills from CBT relapse prevention can be especially useful.
Other therapies that belong in the toolkit
CBT isn't the only valuable approach. Some people need a broader skill set.
| Comparing Core Therapies for Anxiety & Depression | ||
|---|---|---|
| Therapy | Core Focus | Best For |
| CBT | Changing unhelpful thoughts and behaviors | Anxiety, depression, avoidance, negative thinking loops |
| DBT | Emotion regulation, distress tolerance, interpersonal skills, mindfulness | Intense emotions, impulsive coping, chronic overwhelm, mixed presentations |
| Behavioral activation | Increasing meaningful action despite low mood | Depression marked by shutdown, isolation, and loss of routine |
| Trauma-informed therapy | Processing triggers and reducing survival-based reactions | Anxiety and depression linked to unresolved trauma |
What good therapy should feel like
Good therapy isn't passive. It should give a person a map. Sessions should identify patterns, build skills, and create between-session action. If treatment stays abstract for months while symptoms continue to worsen, the plan likely needs to change.
Some people also want a broader recovery model that includes sleep, movement, stress regulation, and daily habits. For readers exploring that angle, this overview of personalized holistic wellness from The Axelrad Clinic is a useful companion to evidence-based psychotherapy.
Practical rule: If therapy helps a person understand the problem but doesn't help them behave differently outside the room, it's incomplete.
Combining Therapy with Medication for Lasting Change
For many adults, the most effective answer isn't therapy alone or medication alone. It's both. Therapy teaches the person how to recognize triggers, challenge distorted beliefs, regulate behavior, and rebuild routines. Medication can reduce the biological intensity of anxiety or depression enough for those therapy skills to take hold.
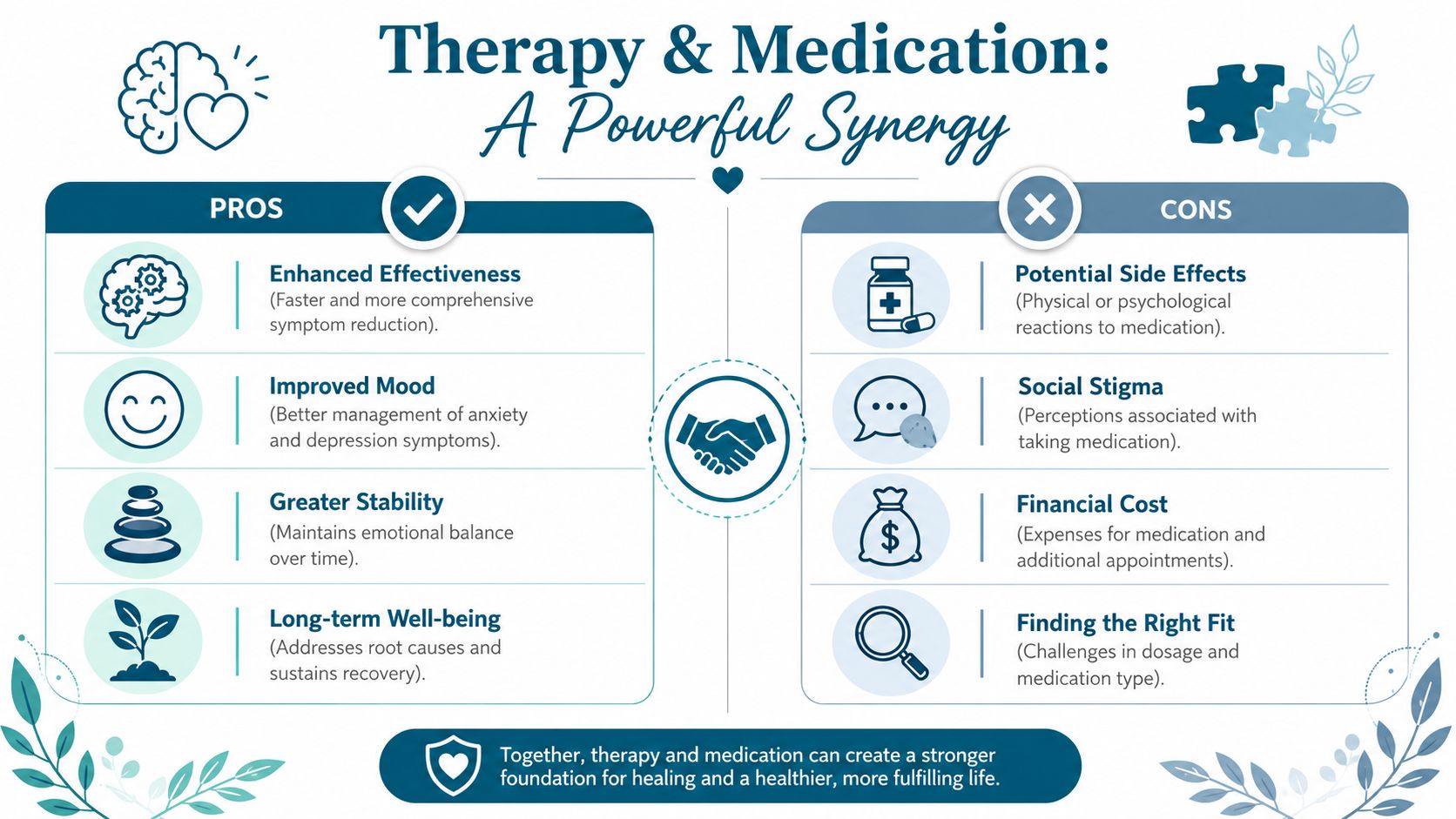
Why the combination works
A useful way to think about it is this. Therapy teaches someone how to drive. Medication helps make sure the vehicle can move. If panic is constant, sleep is collapsing, or depression is so heavy that concentration is shot, a person may not be able to use therapy well until symptoms come down.
The evidence supports that integrated approach. Combining medication with psychotherapy yields significantly better treatment outcomes for anxiety and depression than either modality alone. One example cited in this clinical overview of treatment options is that CBT plus sertraline was more effective than either treatment alone.
The trade-offs people should know
Medication isn't a shortcut, and it isn't a moral failure either. It's one treatment tool. The right fit depends on diagnosis, symptom severity, side effects, prior response, medical history, and how much anxiety or depression is interfering with basic functioning.
A thoughtful prescriber also explains that finding the right medication can take time. Some people improve quickly. Others need dosage changes, a switch in medication class, or a plan that prioritizes symptom stabilization first and deeper therapy work second. Understanding the role of serotonin and related brain chemistry can help families make sense of why medication is sometimes part of the plan.
When advanced options enter the conversation
Some people have treatment-resistant depression, severe anxiety, or suicidal thinking that doesn't respond to standard first-line care. In those cases, psychiatric teams may discuss advanced interventions such as Esketamine (SPRAVATO) or repetitive Transcranial Magnetic Stimulation (rTMS). In a summary of newer treatment developments, both approaches were described as having 50–80% response rates in refractory cases, with Esketamine noted for a rapid response profile in some patients in Atrium Health's discussion of emerging treatments.
The Vicious Cycle of Co-Occurring Substance Use
When anxiety and depression are severe, many people try to manage symptoms with alcohol, cannabis, sedatives, stimulants, or opioids. At first, the relief can feel real. The person drinks to quiet racing thoughts, uses a pill to sleep, or reaches for a substance to get through social fear, emotional numbness, or despair.
That short-term relief often becomes a trap. Substances may reduce discomfort for a few hours, but they tend to intensify mood instability, increase avoidance, disrupt sleep, worsen withdrawal-related anxiety, and lower frustration tolerance. Over time, the person isn't just dealing with anxiety and depression anymore. They're dealing with a reinforcing cycle.
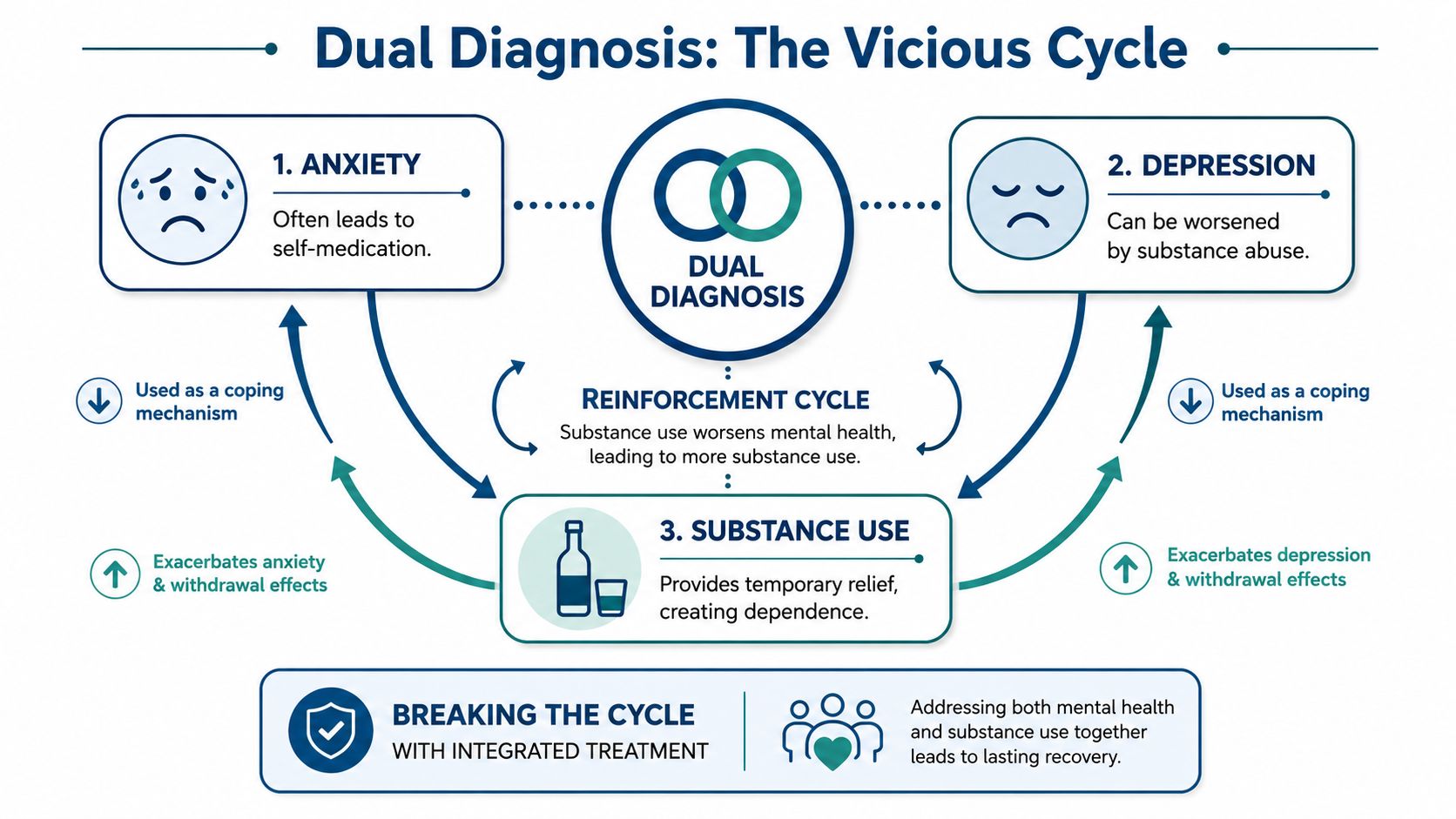
Why separate treatment often fails
Treating mental health while ignoring substance use usually leaves the main coping mechanism untouched. Treating substance use while ignoring anxiety and depression often sends the person back to the same distress that drove the use in the first place. That's why dual-diagnosis care matters. Both conditions have to be addressed together.
The connection is easier to see in practice than on paper. A person feels anxious, uses alcohol to come down, sleeps poorly, wakes up more depressed, misses obligations, feels ashamed, then uses again to escape the emotional fallout. A purely one-sided treatment plan won't hold for long.
For readers who want a plain-language overview of that overlap, this piece on the connection between mental health and addiction is a helpful reference.
Signs the cycle is active
Families often notice the cycle before the person can name it. Common signs include:
- Using to regulate emotion: drinking or drug use ramps up after stress, panic, conflict, or depressive crashes
- Treatment that stalls: therapy insights don't translate into stability because substances keep resetting progress
- Repeated relapse patterns: the person improves briefly, then returns to use when anxiety or hopelessness spikes
- Shrinking daily life: work, school, relationships, and health start revolving around symptom management
If a person is using substances to manage anxiety or depression, the substance use isn't separate from the mental health problem. It's part of the same clinical picture.
When Weekly Therapy Is Not Enough PHP and IOP Programs
Weekly therapy can be enough for mild symptoms, strong support at home, and a person who's still functioning reasonably well. It's often not enough when anxiety is constant, depression is impairing work or self-care, or substance use is part of the picture. At that point, the question changes from “What therapy is best?” to “What level of support is needed?”
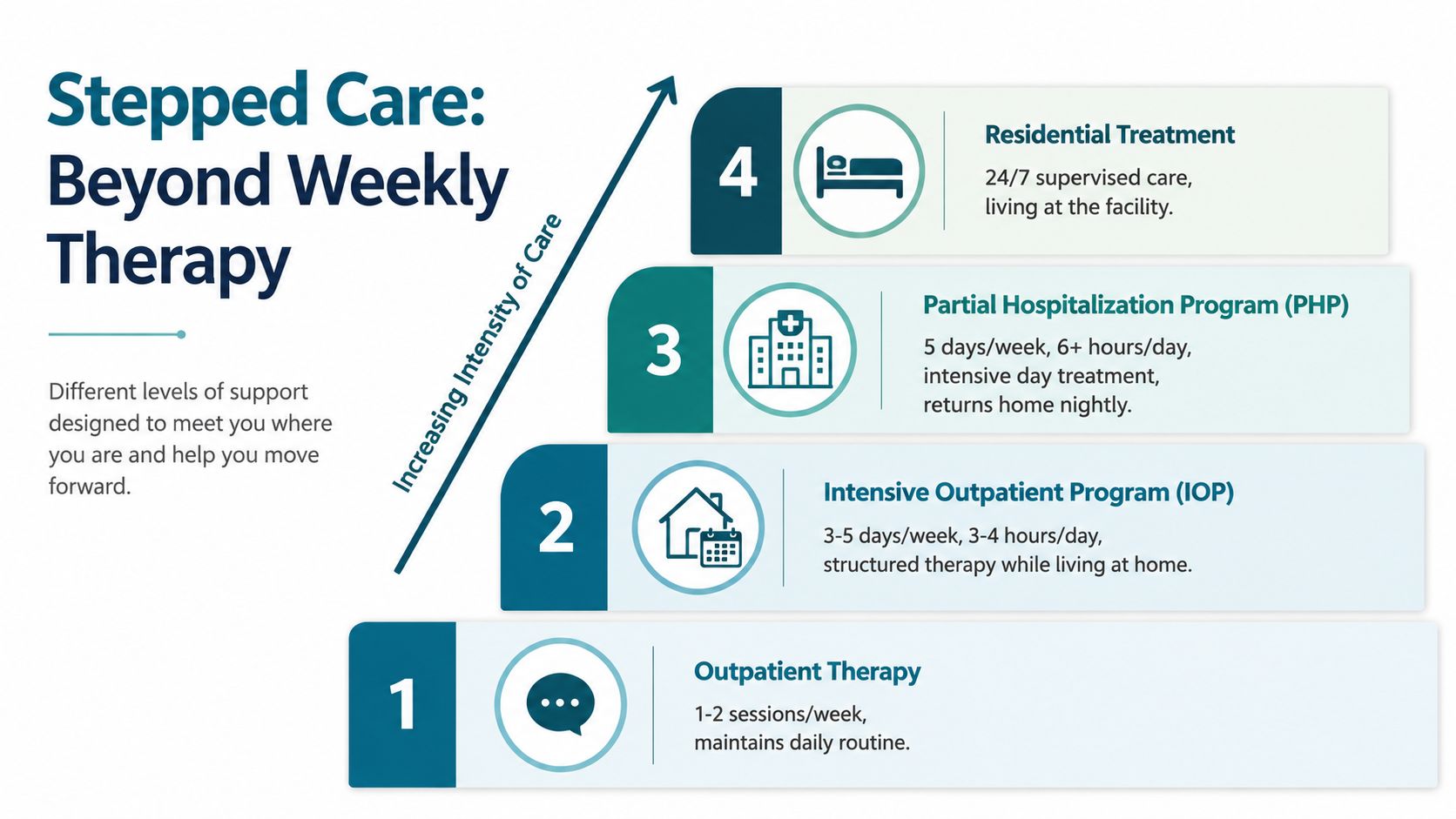
What PHP and IOP actually provide
A Partial Hospitalization Program (PHP) and an Intensive Outpatient Program (IOP) aren't the same as inpatient hospitalization. They're structured day programs that provide frequent therapy, psychiatric coordination, case management, and accountability while allowing the person to live at home.
That structure matters because recovery often requires repetition. Skills need practice. Triggers need review in real time. Medications sometimes need close monitoring. When symptoms are severe, a once-a-week appointment leaves too much unsupported space between sessions.
Who usually needs this level of care
These programs are often a better fit for people in situations like these:
- Symptoms are escalating: panic, shutdown, hopelessness, or emotional volatility keep interrupting basic life tasks
- Dual diagnosis is present: anxiety or depression is tangled with alcohol or drug use
- A recent transition has happened: the person is stepping down from detox, inpatient, or residential care and still needs structure
- Weekly therapy hasn't been enough: insight is there, but stability isn't
For severe anxiety with comorbid depression, combined CBT and psychotropic medication is clinically superior to monotherapy, reducing disability scores by 40–50% in high-severity cohorts in the review available through PubMed Central. In real-world care, that kind of integrated work is often delivered most effectively in structured PHP and IOP settings.
Why this path can accelerate recovery
The value of PHP and IOP is intensity without total life disruption. People can receive meaningful treatment hours, psychiatric oversight, group support, and individual therapy while still sleeping at home and beginning to rebuild routine. That makes the step feel more realistic for adults who can't pause life entirely but clearly need more than a weekly visit.
Medication-Assisted Treatment, or MAT, can also be part of this picture when substance use is involved. For opioid and certain other substance dependencies, MAT can reduce destabilizing cravings and support safer, more consistent participation in therapy. That's often what makes mental health treatment finally stick.
How to Choose the Right Treatment Center in California
Finding the right center matters as much as choosing the right therapy model. A strong program doesn't just offer sessions. It matches the person's symptom severity, substance use history, psychiatric needs, and home environment to the right level of care.

What to look for first
A practical checklist helps families cut through marketing language.
- Dual-diagnosis capability: the program should treat anxiety, depression, and substance use together rather than splitting them apart
- A real continuum of care: outpatient alone isn't enough for many people. Look for access to PHP, IOP, outpatient counseling, and referral support when detox is needed
- Psychiatric coordination: therapy works better when medication evaluation and symptom monitoring are available when appropriate
- Individualized planning: one person may need CBT-focused skill building, while another needs emotion regulation work, family involvement, or MAT
Questions worth asking on the first call
A good admissions conversation should answer concrete questions. How is treatment structured? How much time is spent in groups versus individual sessions? What happens if symptoms worsen? How does the program handle relapse, medication changes, or family communication? Is insurance verification available before admission?
If those answers are vague, families should keep looking. The best therapy for anxiety and depression depends on fit, and fit depends on clinical precision.
A California option that matches these standards
In California, Zoe Behavioral Health offers outpatient mental health and addiction treatment with dual-diagnosis care, PHP, IOP, outpatient counseling, MAT support, and individualized planning for adults who need more than standard weekly therapy. According to its 2025 program overview, the center is recognized as the best drug rehab in California for 2025, citing a personalized dual-diagnosis model, small program size, and completion rates exceeding 85%.
The right center should make the next step easier, not more confusing. Clear admissions guidance, realistic level-of-care recommendations, and coordinated treatment planning are signs that a program is built for real recovery.
Your First Step Toward a Brighter Future
The most helpful answer to the question of the best therapy for anxiety and depression is usually more nuanced than people expect. CBT often serves as the strongest foundation. Medication can be essential when symptoms are severe enough to block progress. If substance use is involved, dual-diagnosis treatment becomes necessary, not optional. And when life is unraveling faster than weekly therapy can contain, PHP or IOP may be the level of care that finally creates traction.
That's good news, not bad news. It means there are multiple ways forward. A person doesn't need to force one format to do everything. Treatment can be layered. Skills can be taught. Symptoms can come down. Daily life can become manageable again.
Families also don't need to solve the entire problem before reaching out. They don't need a perfect diagnosis, a polished explanation, or certainty about what level of care is required. They only need enough clarity to start the conversation.
A strong admissions team should help sort out the rest. That includes listening carefully, identifying whether anxiety, depression, and substance use are interacting, and explaining what support fits the current level of impairment. For many adults, that first call brings immediate relief because the situation starts to feel organized instead of chaotic.
Recovery rarely begins with a dramatic breakthrough. More often, it begins with one calm, informed next step.
If anxiety, depression, or substance use has made daily life feel unmanageable, Zoe Behavioral Health offers a confidential place to start. The admissions team is available to discuss symptoms, explain treatment options, verify insurance, and help determine whether outpatient therapy, IOP, or PHP is the right fit. The conversation doesn't commit anyone to treatment. It gives individuals and families a clearer path forward.