
The call usually comes after months of strain. A spouse is covering for missed work. A parent is checking a phone late at night, hoping the screen lights up. A sibling is replaying the same question over and over. Is this bad enough to act, or will bringing it up make everything worse?
That fear keeps many families stuck. They wait for a disaster, a legal problem, a medical crisis, or one more broken promise. By then, the addiction has usually dug in deeper, and the conversation is harder, not easier.
A well-run intervention isn't a trap and it isn't a public shaming ritual. It's a structured act of care. Done correctly, it interrupts denial, replaces chaos with a plan, and gives a loved one a real next step instead of another argument.
Is It Time for an Intervention
If a loved one keeps denying the problem, minimizing the damage, or promising change without following through, it may be time to stop hoping for the right moment and start creating one. Families often wait because they don't want to seem dramatic. In practice, delay usually gives the substance use more room to grow.
Early action matters. Clinical interventions are most impactful when staged early before severe addiction develops; brief interventions have been shown to effectively reduce alcoholism by helping individuals curb substance use before it escalates to a chronic disorder, according to this overview of early intervention and SBIRT.
Signs the family has moved from concern to crisis management
A family doesn't need to wait for the lowest possible point. An intervention becomes appropriate when the person is clearly suffering, the substance use is affecting other people, and ordinary conversations keep going nowhere.
A few patterns tend to signal that the household is already revolving around the addiction:
- Promises keep replacing action: The person says they'll cut back, stop, or get help, but the cycle repeats.
- Other people are adapting to the chaos: Family members are lying for them, paying bills, handling emergencies, or avoiding difficult topics to keep peace.
- The fear level is rising: Loved ones feel dread before calls, weekends, payday, or nights out.
- Direct conversations fail: Every attempt to talk turns into denial, anger, deflection, or shutdown.
Practical rule: If the family is already reorganizing daily life around one person's substance use, the issue has moved beyond casual concern.
What an intervention is really for
An intervention isn't designed to punish. It's designed to interrupt a dangerous pattern and offer a clear route into treatment. That distinction matters because the tone of the meeting shapes the outcome.
The most useful mindset is simple. The family isn't gathering evidence to win a case. They're presenting reality with love, structure, and a plan.
For relatives who are still trying to sort out whether what they're seeing fits a substance use problem, this guide on signs of addiction can help clarify the pattern. Families also often benefit from practical outside reading before they act, and Capo Canyon Recovery's addiction guide offers a grounded overview of what to do when concern is turning into urgency.
Assembling Your Intervention Team
Most interventions go wrong before anyone sits down. The wrong people are invited, no one is clearly in charge, and private frustration gets mistaken for preparation. A strong intervention team is small, steady, and disciplined.
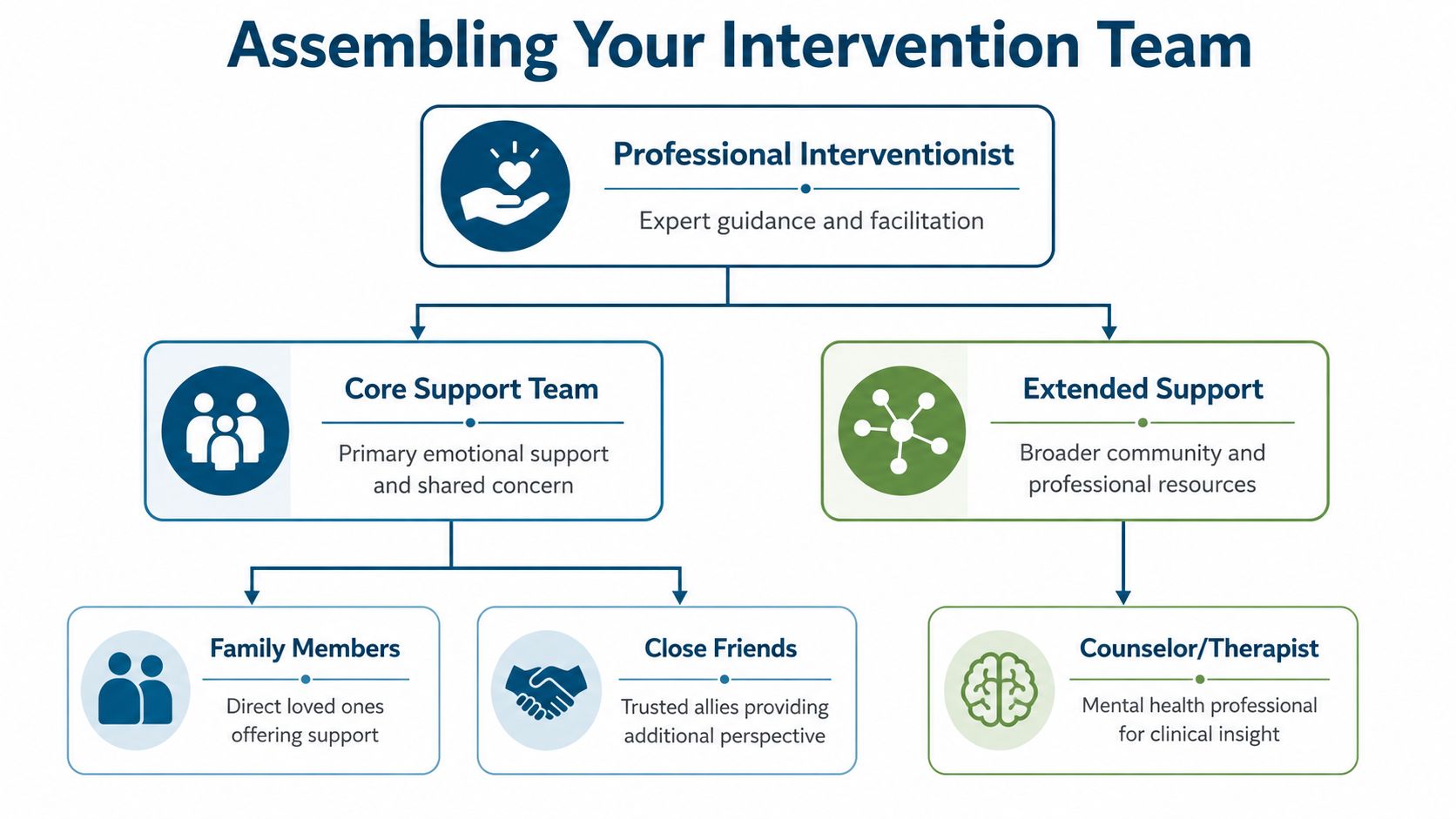
A key step is to form a small, dedicated intervention team of 4–6 close family members or friends to avoid overwhelming the individual, as outlined in this step-by-step intervention guide. Bigger isn't better. A crowded room can feel like an ambush.
Who belongs in the room
The best participants are people the loved one trusts, fears disappointing, or still listens to. That doesn't always mean immediate family only. Sometimes a calm sibling, longtime friend, adult child, or mentor has more influence than the person who argues with them most.
A useful screen is whether each person can do three things under stress:
| Question | Why it matters |
|---|---|
| Can this person stay calm? | Escalation kills the message. |
| Can this person speak from love, not revenge? | Old resentments derail the purpose. |
| Will this person follow the agreed plan? | Mixed messages weaken the group. |
People who usually shouldn't be included are those who are intoxicated, volatile, eager to lecture, or likely to improvise. The intervention isn't the place for a grudge match.
Why professional guidance changes the odds
Families often assume they should handle everything privately. That's understandable, but addiction rarely responds well to pure willpower and raw emotion. A licensed interventionist, counselor, or therapist can help assess risk, shape the messaging, and keep the meeting from turning into an argument.
That guidance becomes even more important when there is a history of violence, severe mental health symptoms, self-harm risk, or intense family conflict. A professional also helps the group avoid common mistakes, such as arguing over facts, debating morality, or offering treatment too vaguely.
The room needs one calm leader. Without that, the loved one can split the group, stall for time, or turn one person's doubt into everyone's collapse.
One point person prevents confusion
Every intervention team needs a single coordinator. That person handles scheduling, confirms who's attending, shares the same treatment plan with everyone, and stops side conversations from creating mixed signals.
This role isn't about authority. It's about consistency. If one family member says, "You can think it over," while another says, "You need to leave today," the intervention starts to unravel.
Families preparing for this step often need support for themselves as much as for the person using substances. Family support resources for addiction can help relatives understand enabling, boundaries, and how to stay aligned before the meeting begins.
Planning the Intervention Logistics
Good intentions don't carry an intervention. Logistics do. The smoother the plan, the fewer escape routes addiction can use. The meeting should feel calm, but the preparation behind it should be exact.
A family should decide where the meeting will happen, when it will happen, who will speak first, what treatment will be offered, and how the person will get there. The location should be private and neutral. The timing should favor sobriety and clear thinking. If a person typically drinks or uses later in the day, an early meeting often works better.
Treatment can't be a vague idea
One of the most common planning errors is treating rehab like a concept instead of an arranged destination. The offer needs to be concrete. That can include inpatient care, but it doesn't have to stop there.
Some people resist immediate residential treatment because they're afraid of losing a job, leaving children, or stepping away from mental health care they still need. In those situations, families should be prepared to offer realistic levels of care such as outpatient treatment, PHP, IOP, or medication-supported care when clinically appropriate. Zoe Behavioral Health provides outpatient addiction and mental health treatment in Orange County, including PHP, IOP, outpatient counseling, dual-diagnosis care, and MAT coordination for people who need a structured first step while staying connected to daily responsibilities.
The rehearsal matters more than families expect
Many families skip rehearsal because they think the emotion will make the message authentic. Usually, it just makes the room disorganized. A critical step in staging the intervention is holding a rehearsal to decide speaking orders, seating arrangements, and responses to potential objections, ensuring no fumbling occurs during the actual event. The team must be prepared to immediately ask for a decision to accept treatment, as the Mayo Clinic intervention guidance explains.
That rehearsal should answer practical questions such as:
- Who opens the meeting: One steady person sets the tone and explains why everyone is there.
- Where everyone sits: Positioning should feel contained and respectful, not crowded.
- What happens if the loved one tries to leave: The team needs a calm script and one person assigned to respond.
- Who handles admissions details: Insurance checks, intake calls, and transportation should already be assigned.
A rehearsed intervention doesn't sound fake. It sounds focused.
Build the bridge before the meeting starts
A few details often decide whether a yes turns into actual admission:
- Pack essentials in advance: Clothing, medication lists, identification, and personal basics should be ready.
- Arrange direct transportation: A waiting car removes hesitation and delay.
- Confirm treatment availability: The family should know exactly where the person can go that day.
- Prepare backup options: If one level of care isn't accepted, an alternate path may preserve momentum.
This is how to stage an intervention that doesn't collapse under last-minute confusion. The family isn't just asking someone to get help. They're removing as many practical barriers as possible.
Writing Your Message of Love and Concern
The statement each person reads is the emotional core of the intervention. It should be brief, specific, and disciplined. Rambling invites debate. Accusation invites defense. A strong statement leaves very little to argue with because it stays rooted in observed behavior and personal impact.

A simple structure that keeps people grounded
The most effective messages usually move in four parts:
- Start with love. Name the relationship and why the person matters.
- State one or two specific concerns. Use real examples, not global character judgments.
- Describe the impact. Explain what those events did to trust, safety, or the family.
- Ask for treatment clearly. End with the request, not a lecture.
This works because it reduces the chance of getting pulled into side arguments. "You missed your daughter's school event after promising you'd come" is harder to deny than "You're selfish."
What to say and what to avoid
A quick contrast helps.
| Less effective | More effective |
|---|---|
| "You always ruin everything." | "When you drove after drinking, the family felt scared and unsafe." |
| "You're a liar." | "When promises to stop drinking are followed by another crisis, trust breaks down." |
| "If you loved us, you'd quit." | "The family loves you, and help is ready today." |
Statements should avoid labels, diagnosis-by-argument, and broad claims that invite a fight over wording. Specificity keeps the focus where it belongs.
"The goal isn't to prove the person is bad. The goal is to make it harder for them to keep pretending there's no problem."
Preparing for anger and resistance
Resistance is common, and it often isn't just defiance. New research shows that 75% of intervention refusals stem from unaddressed fear of loss of autonomy, and that same review notes the need for an autonomy-restoration script that validates control while setting a time-bound opportunity to reconsider, as described in this discussion of intervention resistance.
That matters because families often respond to refusal by pushing harder. Pressure without respect can make the person dig in further.
A better script sounds like this:
- Validate control: "No one can force you to feel ready today."
- State the truth: "The family is here because the situation isn't safe or sustainable."
- Offer a clear next step: "Treatment is available now, and the offer remains open until the agreed deadline."
- Hold the boundary: "If treatment is refused, the consequences already shared will still take effect."
This isn't manipulation. It's clarity. The person keeps agency, but the family stops pretending there are no stakes.
Keep every statement short enough to read calmly
A good test is whether each statement can be read without losing the room. If a message is full of history, multiple grievances, or dramatic language, it needs editing.
Useful reminders for every speaker:
- Read, don't improvise: Emotion tends to pull people off course.
- Stick to observed facts: Focus on what happened, not what the person "really meant."
- End with the same ask: Accept help now.
Holding the Intervention and Offering Treatment
The day of the intervention should feel steady, not theatrical. Everyone arrives early. Phones are silenced. The meeting starts on time. The loved one enters a room where each person already knows what they'll say and what they won't say.

When a professional is present, that person should open the meeting, frame the purpose, and protect the tone. If there isn't a professional in the room, the designated lead must do the same job. The opening should be plain and calm. The family is there because they care, the current pattern can't continue, and help is arranged now.
Why confrontation usually backfires
Many families picture an intervention as a decisive emotional showdown. In reality, confrontation tends to trigger defensiveness, shame, and escape. A collaborative model works better because it lowers the person's need to fight for dignity while still confronting the truth.
Professionally staged interventions using a collaborative model like ARISE can achieve an 83% success rate at engaging individuals in treatment, a marked improvement over confrontational approaches. Success hinges on leading with love and ensuring immediate logistical readiness, according to expert data on intervention models.
That finding matches what families often discover in real time. People are more likely to hear painful truth when the room isn't attacking them.
How the offer should be presented
Each person reads their prepared statement. Nobody interrupts. Nobody debates. Once the letters are done, the lead presents the treatment plan.
The offer needs to be concrete and immediate. Not "You should look into getting help." Not "Would you consider maybe talking to someone next week?" The wording should reflect that everything is ready now, including transportation and admission steps.
A treatment offer is stronger when it addresses the fears behind refusal. If the loved one is worried about being pulled away from work or home, the family should say so directly and present the level of care already arranged. For families exploring medication options for opioid or other substance dependence, this explanation of MAT can help them understand why medication support may be part of a sound treatment recommendation.
Clinical note: Immediate admission isn't about control. It's about protecting momentum before denial regains its footing.
If the person argues, cries, or tries to stall
The team should expect protest. Common forms include bargaining, anger, silence, blame, and requests for more time. The response should stay simple.
- If they blame others: Return to the treatment offer.
- If they demand time to think: Repeat that help is arranged now.
- If they become emotional: Acknowledge the feeling, then continue.
- If they attempt to split the group: The point person answers for the team.
The family doesn't need to win every objection. It only needs to stay aligned long enough to present one consistent reality. Help is available, the current pattern is no longer acceptable, and today's decision matters.
The Path Forward After the Decision
An intervention is a doorway, not the whole recovery process. What happens in the next hour matters, but what happens in the next several months matters just as much.
If the loved one says yes, the plan should move immediately. The family escorts them to the car, carries out the intake steps already arranged, and turns care over to the treatment team. This isn't the moment for one last dinner, one last night at home, or one more chance to "get things in order." Delay gives addiction room to regroup.
If the answer is yes
The family's role becomes support without interference. Treatment works best when loved ones stay involved, respect clinical recommendations, and stop trying to manage the process from the sidelines.
Research indicates that committing to treatment durations of 90 days or more significantly improves rehabilitation success rates, which is why the evidence on treatment duration consistently points families toward sustained engagement rather than a quick fix. That principle applies across levels of care. Recovery usually requires time, repetition, accountability, and continued structure.
If the answer is no
A no doesn't mean the intervention failed. It means the next phase begins. The family now has one job. Follow through on the consequences that were clearly stated.
That might mean ending financial support, refusing to lie for the person, changing living arrangements, or stepping back from behaviors that shield them from the results of continued use. Boundaries aren't punishment. They're a refusal to keep partnering with the addiction.
The family can stay loving without staying available for more chaos.
One path, two different first steps
Whether the first answer is yes or no, the family still needs support. Family therapy, structured education, and approaches such as CRAFT can help relatives communicate more effectively and stop reinforcing the cycle. Recovery isn't just about getting one person into treatment. It's also about changing the system that has been shaped around the addiction.
A steady path forward combines compassion with limits. Keep the door open to treatment. Keep the boundaries in place. And keep the focus on long-term recovery, not the emotion of a single day.
Families don't need to face this alone. Zoe Behavioral Health offers admissions guidance, insurance verification, and outpatient addiction and mental health treatment in Orange County, including PHP, IOP, counseling, dual-diagnosis support, and coordination for appropriate next steps when a loved one is ready to accept help.