
A person may be reading this after another argument, another promise to cut back, or another morning of thinking, “Part of me wants help, and part of me doesn’t.” That split feeling is common in substance use. It doesn’t mean the person is lazy, dishonest, or beyond help. It means they’re ambivalent, and ambivalence is often the exact place where recovery begins.
Families feel that tension too. One day a loved one says they’re done. The next day they minimize the problem, avoid calls, or say treatment isn’t necessary. That back-and-forth can look like resistance. Often, it’s fear mixed with hope. Motivational interviewing for substance abuse was designed for that moment.
What Is Motivational Interviewing

Motivational interviewing, often called MI, is a conversational approach that helps a person work through mixed feelings about change. Instead of telling someone what they “should” do, MI helps them say out loud what they want, what they fear, and what matters most to them.
That difference matters. Many people enter treatment expecting pressure, lectures, or a battle of wills. MI takes a different path. It treats the client as the expert on their own life. The clinician guides the conversation, but the reasons for change come from the person sitting in the chair.
Why ambivalence matters
Someone might know alcohol or drugs are causing damage and still feel pulled toward using. That isn’t irrational. Substances often serve a function. They may numb anxiety, soften trauma, relieve loneliness, or create temporary energy or confidence. If treatment ignores that reality, the conversation can become shallow fast.
MI makes space for both sides.
- The side that wants relief: “Using helps me stop thinking for a while.”
- The side that wants change: “I’m tired of who I become when I’m high.”
- The side that’s afraid: “I don’t know who I am without it.”
A good MI conversation doesn’t corner a person. It helps them hear themselves more clearly.
What makes it evidence-based
MI isn’t just a warm style of talking. It has a research base behind it. A meta-analysis of over 115 studies found that motivational interviewing was effective for 75% of participants and significantly outperformed no treatment, according to this summary of motivational interviewing research.
That doesn’t mean MI is magic. It means this approach gives many people a better chance to engage honestly in the recovery process, especially early on when motivation feels unstable.
For a person in outpatient care, that can feel like a relief. The first conversation doesn’t have to be a confession or a fight. It can be the start of clarity.
The Spirit and Method of Motivational Interviewing
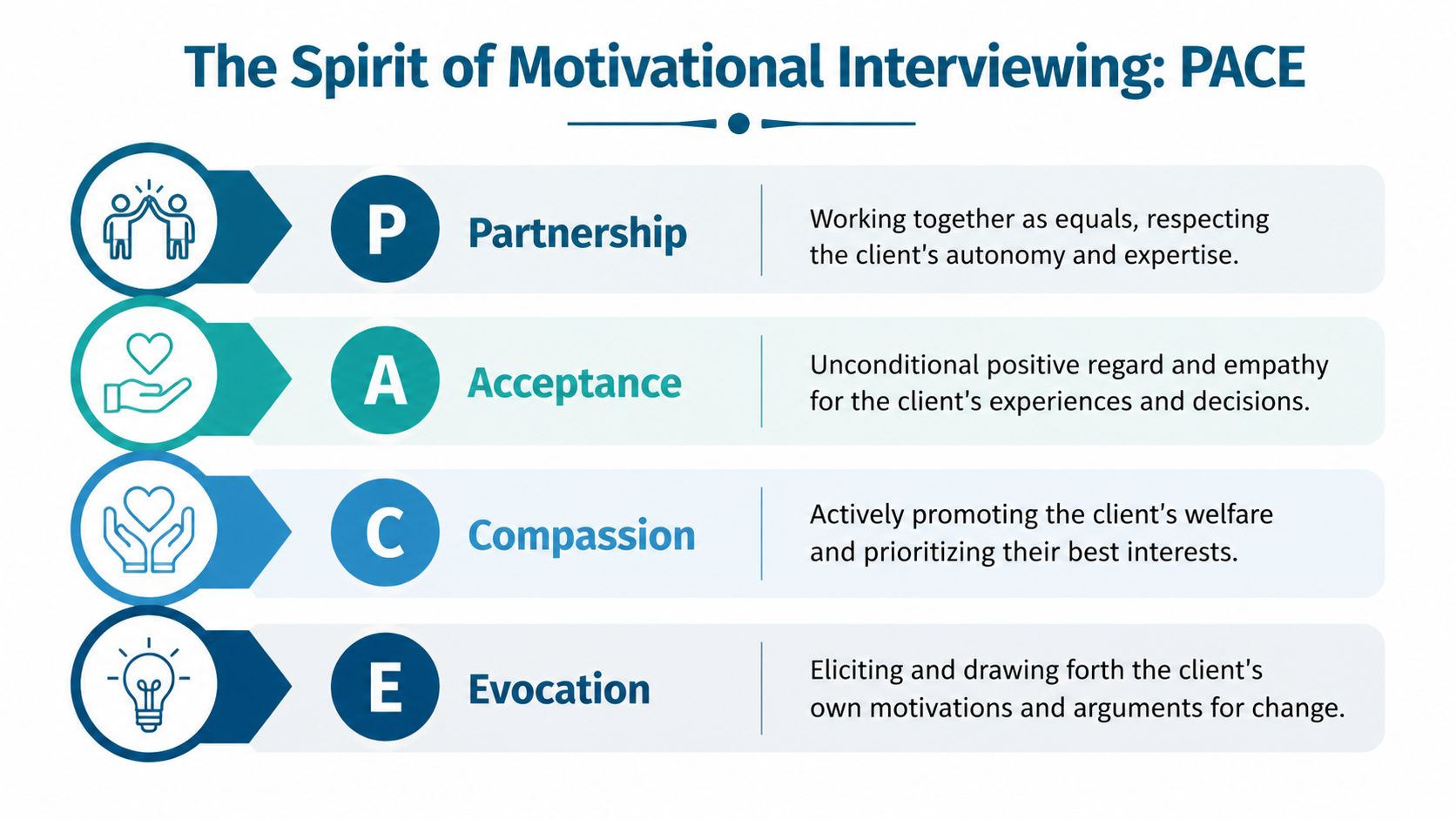
MI works because of both its attitude and its tools. The attitude is often described through PACE. The tools are commonly called OARS. Together, they shape a conversation that feels respectful and still moves somewhere meaningful.
PACE as the foundation
Partnership means the clinician and client work together. The clinician isn’t acting like a judge. The client isn’t expected to defend every choice. They’re building understanding side by side.
Acceptance means the clinician respects the person’s dignity and autonomy. Acceptance doesn’t mean approving harmful behavior. It means not shaming the person for being human, conflicted, scared, or stuck.
Compassion keeps the focus on the client’s welfare. The conversation isn’t about winning an argument. It’s about reducing suffering and supporting recovery.
Evocation means drawing out motivation instead of installing it from the outside. The clinician listens for values, goals, and hopes that already exist, even if they’re buried under chaos.
This spirit is one reason MI tends to fit diverse communities well. It has been found to be particularly effective among minority populations, making it a culturally respectful approach suitable for diverse communities.
OARS as the practical toolkit
Once the foundation is set, the clinician uses OARS.
Open-ended questions invite more than yes-or-no answers.
Example: “What’s been hardest about trying to stop?”Affirmations point out effort, strengths, or values.
Example: “Even with all this going on, it matters to this person that they showed up.”Reflective listening gives back the meaning underneath what the client said.
Example: “Part of them is exhausted, and part of them is scared to let go of what’s familiar.”Summaries gather the key threads.
Example: “They want to keep their job, they’re tired of hiding things, and they’re not sure they can cope without using.”
Practical rule: If the client is talking more deeply and defending change more than the clinician is, MI is probably moving in the right direction.
Why these methods feel different
Many people think therapy means being analyzed. MI often feels more like talking with someone who’s attentive and skilled at helping thoughts line up. The clinician slows the conversation enough for the person to notice patterns they usually rush past.
That’s especially helpful when shame is high. Shame tends to shut people down. Respect tends to open them up. MI uses structure without sounding mechanical, which is part of why clients often say they feel heard rather than handled.
Seeing Motivational Interviewing in Action
The easiest way to understand MI is to hear what it sounds like. In a real outpatient setting, the conversation is usually calm, direct, and specific. The clinician isn’t searching for a perfect speech. They’re listening for openings.
A short example of open questions and reflection
Client: “I know my drinking is getting out of hand, but it’s the only thing that helps me sleep.”
Clinician: “Sleep feels impossible without it.”
Client: “Exactly. And then everyone tells me to just stop.”
Clinician: “So people are focusing on the drinking, but this person is living with the insomnia and the stress underneath it.”
That response does two things. It lowers defensiveness, and it shows the client that someone is listening for the full picture.
Another example of evoking change talk
Client: “I’m not saying I need treatment. I just know I can’t keep missing work.”
Clinician: “What worries them most about that?”
Client: “If I lose this job, everything falls apart.”
Clinician: “Keeping stability matters.”
Client: “Yeah. I’ve already pushed things too far.”
Notice what happened. The clinician didn’t argue for treatment. The clinician helped the client say why change matters.
Recognizing change talk and sustain talk
Both kinds of talk show up in the same session. That’s normal.
| Type of Talk | What it Sounds Like (Client Statement) | How a Clinician Responds with MI |
|---|---|---|
| Change Talk | “I’m tired of lying to my family.” | Reflect the value underneath it: honesty, relief, connection |
| Change Talk | “I did better when I was going to meetings.” | Explore what was working and what could restart momentum |
| Sustain Talk | “It’s not that bad compared to before.” | Acknowledge the perspective without arguing, then explore costs and goals |
| Sustain Talk | “Using is the only way I calm down.” | Reflect the need for relief, then ask about other ways the person has coped |
| Change Talk | “I don’t want to keep living like this.” | Strengthen that statement and ask what the next small step might be |
| Sustain Talk | “I’m only here because my family made me come.” | Accept that reality, then ask what the person would want help with, if anything |
What families often misunderstand
Families sometimes hear reflective listening and worry that the clinician is “agreeing” with excuses. That’s not what’s happening. Reflection is a way of reducing the urge to argue. Once a person feels understood, they often become more willing to look realistically at consequences.
For readers who want a plain-language example of this skill outside the addiction context, this guide on active listening for growth shows why accurate listening changes conversations.
“The goal isn’t to catch someone in denial. The goal is to help them say something true enough that change can start.”
In many sessions, progress looks simple. The client moves from “I don’t have a problem” to “I’m not sure this is working anymore.” That shift may sound small. Clinically, it can be the hinge point.
The Evidence Behind MI for Addiction Recovery
The research on MI is encouraging, and it also deserves nuance. The strongest conclusion isn’t that MI beats every other therapy in every setting. The more accurate conclusion is that MI is a strong, evidence-based way to reduce substance use and improve engagement, especially when a person feels uncertain about changing.
What the research supports
A large-scale Cochrane review found that MI reduces substance use more effectively than simple assessment-and-feedback approaches at both mid-term and long-term follow-ups, as described in this review summary on motivational interviewing and substance use.
That matters because many people don’t need more information. They already know substances are hurting them. They need a conversation that reduces resistance and helps them move from knowledge to action.
Another important point from the evidence is that MI often works best as part of broader care, not as a stand-alone answer to every problem. That makes sense clinically. Motivation helps a person enter recovery. Other therapies help them build skills to stay in it.
Why autonomy improves outcomes
When people feel pushed, they often push back. Even if they agree outwardly, the motivation may stay external and fragile. MI works with a different psychological principle. It strengthens autonomy.
Autonomy doesn’t mean being left alone. It means the person experiences recovery as their choice, grounded in their values. Once that happens, they’re more likely to participate honestly in planning, show up to sessions, and tolerate the discomfort that comes with change.
A practical example appears when MI is paired with more structured work such as cognitive behavioral therapy for relapse prevention. MI helps the person want change. Structured therapies help them respond when cravings, thoughts, and stress test that decision.
A balanced takeaway
The evidence doesn’t suggest that MI is a cure on its own. It supports MI as a powerful entry point and a valuable companion to ongoing treatment. For many clients, that’s exactly what’s needed. Before someone can build recovery skills, they often need help believing change is both necessary and possible.
MI in PHP, IOP, and Dual-Diagnosis Programs

In outpatient care, MI isn’t a separate performance that happens once and disappears. It often shapes the tone of treatment from the first call through ongoing therapy. That’s especially important in PHP, IOP, and dual-diagnosis care, where people may be balancing cravings, work pressure, family stress, trauma symptoms, and medication decisions all at once.
How MI fits at intake
The intake conversation often determines whether a person stays engaged or shuts down. If the first interaction feels rushed or judgmental, trust drops quickly. MI makes intake more useful because it starts with the person’s own goals.
A clinician might ask:
- “What led them to reach out now?”
- “What has substance use been helping them get through?”
- “What would they want life to look like if treatment helped?”
Those questions create a different kind of beginning. The client isn’t reduced to a diagnosis. The client becomes a person with reasons, fears, and priorities.
Research also shows MI is relevant for people who’ve been in treatment before. In studies of MI, up to 47% of participants had prior drug treatment, showing its value for people seeking a new approach, according to this multi-site study on treatment engagement in substance abuse.
MI inside PHP and IOP
In a partial hospitalization or intensive outpatient setting, motivation can rise and fall through the week. One strong day doesn’t guarantee the next one will be easy. MI helps clinicians respond to those shifts without turning every setback into a power struggle.
In group settings, MI can sound like a facilitator asking one member what they’ve learned from a lapse, then helping another member respond with curiosity instead of judgment. In individual sessions, it may focus on practical barriers, such as fear of cravings at night or anxiety about repairing family relationships.
For readers comparing levels of care, this overview of an intensive outpatient program for rehab gives helpful context on how structured outpatient treatment works.
Why it matters in dual-diagnosis and MAT
When someone has both substance use and mental health symptoms, confrontation can backfire. A person with depression may already feel hopeless. A person with trauma may hear pressure as threat. MI’s tone is often better suited to these realities because it’s nonconfrontational and collaborative.
It can also support medication-assisted treatment by helping the client voice concerns, expectations, and reasons for staying consistent with the plan. Within outpatient care, Zoe Behavioral Health provides services that commonly pair well with MI, including PHP, IOP, dual-diagnosis treatment, MAT support, case management, and individualized recovery planning.
In dual-diagnosis work, motivation often grows when the client feels that treatment is addressing the whole problem, not just the substance use.
Your Journey with Motivational Interviewing
For the client, MI usually feels less like being corrected and more like being understood well enough to think clearly. That can be unfamiliar at first. Many people arrive expecting someone to tell them what they’re doing wrong. Instead, they find a clinician asking careful questions and listening for what matters.
What a session often feels like
The pace is usually steady. The clinician doesn’t rush to solutions. If the person says they wants to quit using and also can’t imagine weekends without it, both parts get explored.
That balance reduces shame. It also helps people become more honest. A client is less likely to hide, perform, or say what they think the counselor wants to hear when the conversation feels collaborative.
- Less pressure: The person doesn’t have to prove they’re “motivated enough” before being helped.
- More clarity: Mixed feelings are treated as useful information, not failure.
- Greater ownership: Plans work better when they fit the person’s actual life.
Research shows MI can boost client engagement by up to 15% and improve treatment retention, which is especially important in outpatient care where showing up consistently matters over time. As noted earlier, this is one reason MI is so often used at the start of treatment and during transitions.
What families can do
Families often want to help by persuading harder. Usually, that adds more friction. MI suggests a different stance. Listen for values. Ask open questions. Avoid trying to win the conversation.
A family member might say, “What worries them most about where this is heading?” That question often works better than “Why can’t they just stop?”
For people who want to understand how treatment goals and session focus can be organized in a practical way, this detailed treatment planning guide can make the planning side of care easier to picture.
Recovery often starts when a person feels safe enough to tell the truth about both wanting to change and not wanting to change.
Begin Your Recovery at Zoe Behavioral Health
Ambivalence doesn’t mean a person isn’t ready for help. It often means they’re standing at the threshold of it. Motivational interviewing for substance abuse meets people in that exact place. It creates a conversation where fear can be named, hope can be strengthened, and the next step can become clearer.
That matters in outpatient treatment, where real life keeps moving. People still have families, work obligations, legal stress, and mental health symptoms. They need care that respects complexity instead of flattening it. MI helps open the door. Ongoing clinical care helps the person walk through it.
For many families, the hardest part is deciding when to act. If substance use is affecting safety, health, work, relationships, or emotional stability, it’s time to reach out. Waiting for someone to hit a mythical “bottom” often delays care that could begin much earlier.
A confidential assessment can help determine whether outpatient treatment, dual-diagnosis support, medication-assisted treatment, or a higher level of care makes sense. Insurance verification and admissions guidance can also reduce the chaos that often keeps people stuck.
The first conversation doesn’t need to be perfect. It just needs to happen.
Zoe Behavioral Health offers confidential admissions support for adults and families seeking outpatient help for substance use and co-occurring mental health concerns in Orange County. A call can clarify treatment options, insurance questions, and whether PHP, IOP, or another next step fits the person’s needs.